



Is your child much shorter – or much taller – than other kids his or her age?
Some children may be small for their age, but still be growing normally, while others are short or tall because their parents are the same.
These children are normal and healthy.
But some children may have growth disorders.
Growth disorders are problems that prevent children from developing normal height, weight or puberty.
Being too short or too tall, or having very slow or very fast growth, can sometimes be due to either nutrition, an underlying medical condition or hormone problems.
Many parents are concerned that their child is short.
A child is defined to be short if he or she is unusually short in comparison to the general population or to their parents.
If your child’s height is below the third percentile line of the sex- and age-appropriate growth chart, then he or she is short in comparison to the general population.
For example, if a child’s height is on the third percentile, this means that only three in 100 children of similar age and sex have a height measurement below this line.
It means the child is among the shortest 3% of children of similar age and sex.
This might not necessarily be a growth problem as a child’s final height is also determined by the height of their parents.
If the child has short parents whose heights sit around the third percentile of the adult height chart, and the child has been growing normally along the third percentile line, then the child is less likely to have a growth problem.
A child who has not been growing at the expected rate, despite having normal height – i.e. their growth shows a downward trend and is dropping down the percentile lines – is a greater cause for concern.
So, how do we know if your child is growing at a normal rate and able to reach their expected final height?
Monitoring growth
Children grow at different, but fairly predictable, rates throughout life.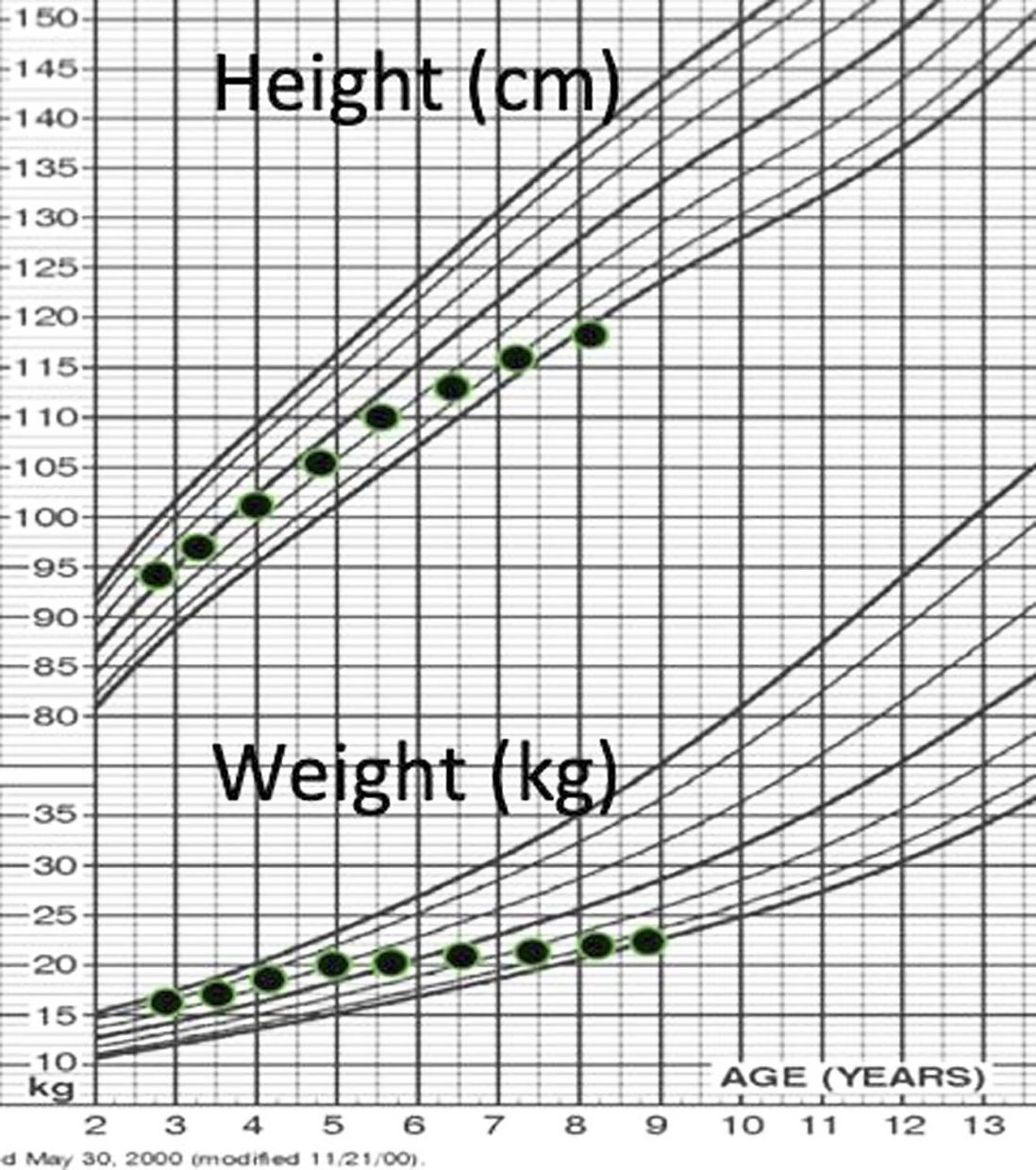
Growth is fastest during the first year of life where babies grown in length at an amazing rate of 25 centimetres a year.
After the infantile phase, the growth rate (growth velocity) slows to a steady rate of 5-7cm per year.
This means that during childhood, a child typically grows 5-7cm per year.
During puberty, there is the pubertal growth spurt, and growth rate increases to about 8-10cm per year.
Puberty usually lasts about two to three years.
After that, the bones mature, growth plates fuse and growth ceases.
A child’s height should be monitored during well-clinic visits to their paediatrician by plotting their measurements on a growth chart.
Regular routine checks should be at least yearly or more frequent in younger children.
By monitoring your child’s height as he or she grows, the doctor is able to look at the growth pattern and determine if the growth rate is normal.
Reasons for short stature
There are many reasons why a child may be short.
A common reason is familial short stature, which means the parents are short.
Maturational (constitutional) delay is another cause, where the child is a late bloomer and catches up during puberty.
Children with familial and maturational short stature often do not need any treatment.
Sometimes, there are medical conditions that lead to poor growth, e.g. poor nutrition; anaemia; bone, heart, kidney, liver or gastrointestinal conditions; poorly-controlled asthma; diabetes; malabsorption or cancer.
Children on medications such as prolonged high-dose steroid therapy, or who have undergone head or spine radiotherapy, may also have poor growth.
Hormone problems such as growth hormone deficiency, hypothyroidism (low thyroid hormones) and Cushing syndrome (excess cortisol hormones) are less common, but are important to keep in mind and diagnose, as they are often treatable.
Children who have delayed puberty are also short, as they do not have their pubertal growth spurt.
On the other hand, children with early puberty, despite an earlier growth spurt, also end up short as their bones mature and fuse faster.
Some children are small because they are born small for gestational age, premature, or have underlying genetic syndromes, e.g. Down, Turner, Russell Silver, Noonan or Prader Willi.
Decisions on treatment depend on the underlying cause, e.g. optimising nutrition and treatment for any underlying medical conditions.
Growth hormone injections are beneficial for some children, e.g children with not enough growth hormones, who are born small for gestational age, or who have certain genetic syndromes such as Turner.
Regular follow-up with a paediatrician and regularly plotting their height on a growth chart is important to ensure early recognition and intervention to help the child achieve his or her genetic height potential.
How can parents help?
There are a few things parents can do to help their child grow normally.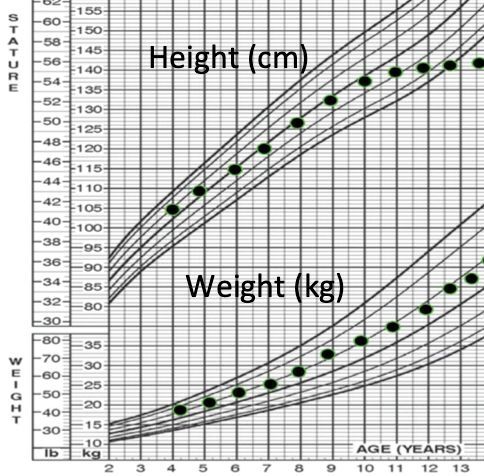
For good health and wellness, children need:
- Enough rest – most young children need an average of 10 to 12 hours of good-quality sleep, and adolescents eight to 10 hours.
- Good nutrition – an appropriate, balanced diet.
- Exercise – enjoyable physical activities or exercises as a family.
If parents are worried about their child, don’t wait until puberty to see if the child will “catch up” on growth.
During puberty, the bones start to mature faster.
At the end of puberty, the growth plates will fuse and not much growth can then be achieved, even if there is a treatable cause.
In most girls, growth and puberty are complete at around 14 years of age (or shortly after their first period), and in boys, 16 years of age.
Therefore, if parents have any concerns that their child’s height is abnormal or that their child is not growing at an expected rate, it is best to bring them to see a medical specialist early.
The following are a few signs that parents should take seriously:
- Their child is shorter compared to his or her friends of the same age and sex.
- Their child does not appear to be growing over a period of time.
- Their child grows less than 5cm per year during childhood to puberty.
- Their child grows less than 7cm per year during puberty.
- Their child shows early signs of puberty, i.e. breast development in girls younger than eight years of age, menses in girls younger than 10 years of age, or testicular/genital enlargement in boys younger than nine years of age.
- Their child shows no signs of puberty at the age of 13 years for girls and 14 years for boys.
Short stature can be an emotional issue among parents and teenagers, who may have different expectations.
While height may have its advantages, height itself does not define the person.
However, severe short stature can affect a person’s self-esteem and their ability to carry out daily activities.
Therefore, if parents have any concerns that their child has a growth problem, it is best to see a paediatrician earlier, rather than later.
Dr Jeanne Wong Sze Lyn is a consultant paediatrician and paediatric endocrinologist. This is the seventh article in a monthly series called Hormones and Kids. For more information, email starhealth@thestar.com.my. The information provided is for educational purposes only and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this column. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


