



Rickets is a preventable condition that causes weak and soft bones in children.
Impaired mineralisation in rickets affects the growth plates in growing bones, resulting in bone deformities such as bowing of the legs, swelling of the wrist and knee joints, and radiographic changes seen on X-rays.
Growth plates are the areas of new bone growth in children.
Most growth plates are located at the ends of the body’s long bones at the thigh, lower legs, forearm, hands and feet.
Rickets is more common in infants and children, but can sometimes occur in teenagers too.
Adults do not develop the bone deformities seen in rickets as their growth plates have already fused.
The diagnosis of rickets is made through taking the patient’s history as related to the condition, clinical findings and blood tests, and is confirmed by the presence of radiographic changes.
The most common type of rickets worldwide is nutritional rickets, which is due to low vitamin D or calcium.
Other types of rickets include heritable disorders of vitamin D metabolism, hypophosphataemic rickets and metabolic bone disease of prematurity (rickets of prematurity).
This article will focus on nutritional rickets.
Kids at risk
Vitamin D comes mostly from exposure to sunlight and some foods like oily fish and eggs.
Some foods may have vitamin D added to it, e.g. cereals, infant formula milk, dairy products or margarine.
This vitamin helps the body absorb calcium and phosphate, which are essential minerals needed to form bones and teeth.
It has other roles in the body as well, including reduction of inflammation and immune function.
Vitamin D deficiency occurs even in tropical countries with abundant sunlight such as Malaysia.
This could be due to various reasons, e.g. dark skin, clothes that limit skin exposure, atmospheric pollution and a lack of vitamin D-fortified foods.
Local studies show a high prevalence of vitamin D deficiency among young Malaysian adolescents, which could be as high as 70%.
Rickets is usually caused by low vitamin D, especially if there is also low calcium intake.
Dietary calcium deficiency is a major cause of nutritional rickets in Asian and developing countries where there is a characteristic low intake of milk and dairy products.
This low calcium intake could be due to various reasons, including poverty and food preference.
Calcium is mostly found in milk and dairy foods.
Rickets is also more likely in babies who are born to mothers with vitamin D deficiency, exclusively breastfed, born premature and late in starting solid foods at the recommended normal age (around six months old).
Children with dairy allergies, or renal, liver or gastrointestinal diseases, are also at risk for rickets.
In high-risk groups, blood parameters on bone, calcium and vitamin D levels may need to be monitored periodically.
Signs and symptoms
A two-year-old boy was brought to see a paediatrician for a waddling gait and progressive bowing of his legs.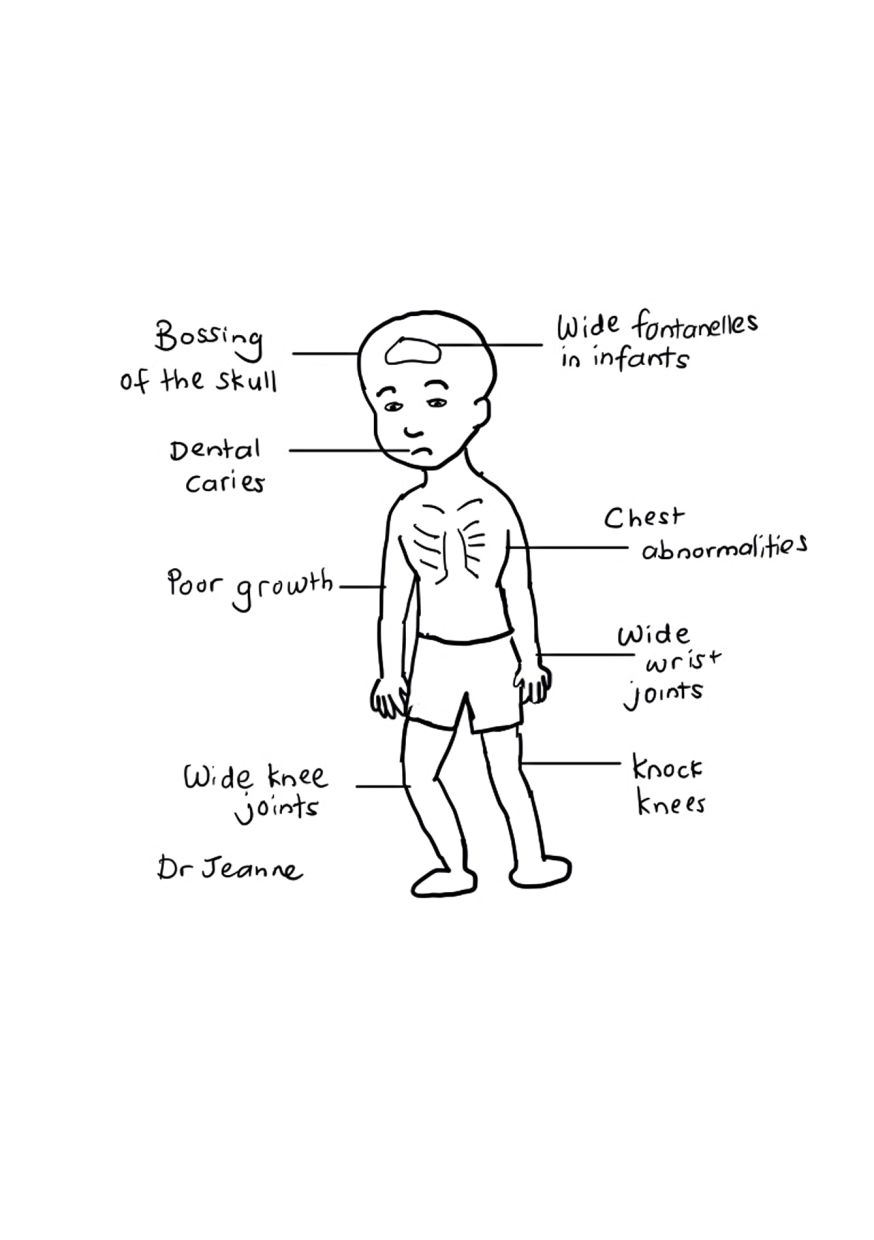
His parents started to notice his legs were bending inwards when he first started walking.
He was described as a picky eater.
Solids were introduced into his diet late and he was predominantly breastfed up to one year of age.
His vitamin D level was low and X-rays showed fraying at the ends of his bones.
He was started on vitamin D supplements (cholecalciferol), while his parents were advised to ensure he had enough dietary calcium.
The bending of his legs soon stopped and they slowly became straighter.
The signs and symptoms of rickets include bone pain; bowed legs; deformities of the chest, wrist and knee joints; poor growth; dental problems, and fractures.
Some babies and children may also have low levels of calcium in their blood (hypocalcaemia), which can cause muscle cramps, twitching, tingling and numbness in the hands and feet.
If the calcium level is very low, seizures can occur, especially in infants.
Severe vitamin D and calcium deficiency can also cause heart failure in babies in a condition known as dilated cardiomyopathy.
Hence, babies and children with very low calcium levels will need admission to the hospital for monitoring.
Vitamin D supplements are given for low vitamin D. A higher dose than usual is required in rickets.
Calcium supplements are often needed initially as well if the blood calcium level is low or if there is inadequate calcium intake from the food.
Preventing rickets
Identifying babies and children who are at risk and addressing the risk factors discussed above can prevent rickets.
These include making sure women who are pregnant take the recommended daily amounts of vitamin D and calcium.
Global consensus guidelines on nutritional rickets recommend vitamin D supplementation of 400 international units (IU) daily for babies from birth to one year of age, especially for those who are exclusively breastfed.
It is advisable however, for babies to be introduced to solid foods from six months of age, which should help provide some vitamin D through their diet.
Older children should get 600 IU of vitamin D per day through their diet and/or supplementation.
Exposure to sunlight provides the best source of vitamin D.
However, such exposure must be done in a safe manner as overexposure can result in overheating, sunburn, eye damage and skin cancer.
Infants and young children should avoid direct sun exposure.
Adequate dietary calcium intake in children is also very important.
Based on the Global Consensus Recommendations on Prevention and Management of Nutritional Rickets, recommended calcium intake for infants aged zero to six months is 200 milligrammes per day, and 260 mg/day for those aged six to 12 months.
Most infants get enough calcium from their milk intake.
For children over one year of age, a sufficient dietary calcium intake is more than 500 mg/day.
This roughly equates to two to three servings of dairy products each day.
An example of one serving of dairy is one glass of milk, one slice of cheese or one tub of yoghurt.
A low calcium intake of less than 300mg in children increases the risk of rickets, regardless of their vitamin D level.
Dr Jeanne Wong Sze Lyn is a consultant paediatrician and paediatric endocrinologist. This is the second article in a monthly series called Hormones and Kids. For more information, email starhealth@thestar.com.my. The information provided is for educational purposes only and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this column. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


