



Similar to adults, babies and children can have thyroid problems too.
However, when the thyroid gland does not work properly in young children, they are at risk of delayed brain development, as well as growth, weight and pubertal problems.
The thyroid gland is a butterfly-shaped endocrine gland located at the front of the neck.
It produces thyroid hormones that play an important role in regulating the body’s metabolism, temperature and heart rate.
In babies and young children, thyroid hormones are critical for brain development and growth.
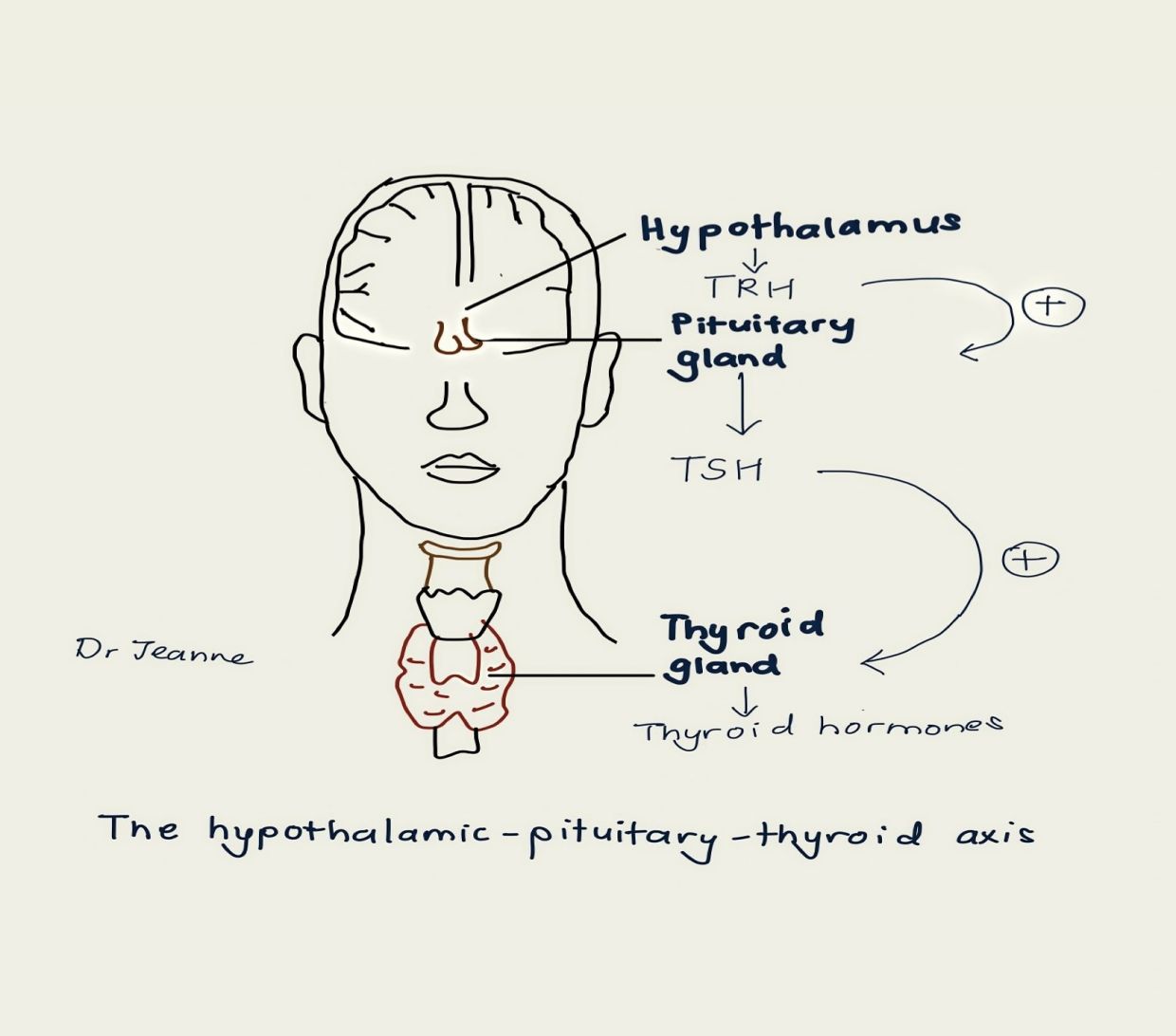
But the production of these hormones depends on more than just the thyroid gland, it is directly influenced by what is known as the hypothalamic-pituitary-thyroid axis.
The pituitary gland is a small gland located at the brain.
It produces thyroid-stimulating hormone (TSH) that signals to the thyroid gland how much thyroid hormone to produce.
TSH levels change according to the body’s needs to produce more or less thyroid hormones.
The pituitary gland responds to signals from the hypothalamus, which sits above it in the brain.
The hypothalamus releases thyrotropin-releasing hormone (TRH), which stimulates the release of TSH from the pituitary gland.
This whole network is the hypothalamic-pituitary-thyroid axis.
The most common thyroid disorders in children are those concerning production of thyroid hormones, i.e. too little production (hypothyroidism) or too much (hyperthyroidism).
Other less common thyroid disorders in children are thyroid nodules, cancer and other rare forms of inherited thyroid disease.
Hypothyroidism
Baby Anne was born healthy and sent home promptly after birth.
However, the third day after she was born, her parents received a call from the doctor saying that her newborn screening test for congenital hypothyroidism was abnormal.
Baby Anne would need thyroid hormone medication and repeated thyroid function tests to monitor her condition.
Unfortunately, times were tough and baby Anne’s father lost his job.
The family moved back to their hometown in a remote area and stopped follow-up for baby Anne.
One year later, she represented to the paediatric clinic with stunted growth and delay in motor skills.
On examination, she was short with coarse facial features, dry skin and poor muscle tone.
Repeated blood tests for baby Anne showed severely low thyroid hormones.
Hypothyroidism, or an underactive thyroid leading to a lack of thyroid hormones, is the most common thyroid disorder in children.
It slows the body’s metabolism.
Clinical features of hypothyroidism in babies and children develop gradually over a period of time and may not be obvious initially.
Diagnosis is made by a simple blood test to check for thyroid hormone concentration.
Common signs and symptoms for hypothyroidism include:
- Delayed development
- Learning difficulties
- Poor growth
- Slow heartbeat
- Cold intolerance
- Constipation
- Weight gain, and
- Goitre (swelling of the thyroid gland at the neck).

Causes of hypothyroidism
Hypothyroidism can be congenital or acquired later in childhood.
Congenital hypothyroidism refers to hypothyroidism that is present at birth.
It occurs when the thyroid gland is underactive, absent or not fully formed.
Central hypothyroidism is a less common form of congenital hypothyroidism, and is due to abnormalities in the hypothalamic- pituitary-thyroid axis.
Since the introduction of newborn screening worldwide in the 1970s, the frequency of congenital hypothyroidism has been calculated to be approximately one in 2,000 to 4,000.
In Malaysia, the incidence of congenital hypothyroidism published in local studies range from one in 1,170 to 3,666 live births.
Frequency is likely to vary based on different screening methods and populations.
Higher cases being reported may be related to lower screening thresholds used, resulting in detection of mild cases.
In Malaysia, the screening test is performed at birth, whereby a small amount of the baby’s cord blood is tested.
In the past, cretinism was a term commonly used to describe infants and children with complications of untreated hypothyroidism, such as coarse facial features, stunted growth and mental retardation as seen in baby Anne.
Now, with early diagnosis and treatment, babies with congenital hypothyroidism will be able to develop normally, both physically and mentally.
Also known as Hashimoto’s disease, autoimmune thyroiditis usually occurs in older children.
In this condition, abnormal antibodies produced by the body mistakenly attack and damage normal thyroid cells.
During the early phase of the disease, the thyroid gland may produce higher amounts of thyroid hormones than normal, resulting in hyperthyroidism.
However, over the weeks and months, the hyperactive phase will pass and the thyroid gland will become underactive, resulting in low thyroid hormones instead, i.e. hypothyroidism.
Children with certain conditions, such as Down syndrome and Turner syndrome, have a predisposition to developing autoimmune thyroiditis and require their thyroid function to be monitored regularly.
Iodine is required for the production of thyroid hormones.
Babies born to mothers with severe iodine deficiency are at risk of poor brain development.
Iodisation of salt or iodine supplementation of bread helps to ensure that populations have enough dietary iodine.
However, excessive iodine can also result in hypothyroidism by affecting the production of thyroid hormones.
Hence, while sufficient iodine is important, it is also unsafe to take large amounts of iodine supplements.
Some drugs, such as amiodarone, aluminium hydroxide, lithium and cholestyramine, can cause hypothyroidism.
Hypothyroidism can also occur after radiation exposure for treatment of brain, head or neck tumours.
These effects are usually transient, but the patient’s thyroid function should be monitored.
Hyperthyroidism
Daniel, 13, presented to the emergency department with chest pain, breathlessness and palpitations that had been going on for two days.
On examination, he was thin with prominent eyes and a neck swelling.
Upon further questioning, his parents revealed that Daniel’s school performance had deteriorated over the past one year.
He had also lost weight despite having a voracious appetite.
His blood test revealed abnormally high thyroid hormones.
He was started on medications to reduce his thyroid hormones and ease his symptoms, especially his accelerated heart rate.
In contrast to hypothyroidism, too much thyroid hormone increases the body metabolism.
Hyperthyroidism, also known as an overactive thyroid or thyrotoxicosis, occurs in approximately one in 5,000 children and adolescents.
Unlike in adults, the presentation of hyperthyroidism in children can be subtle, resulting in a delay in diagnosis, as in the case of Daniel.
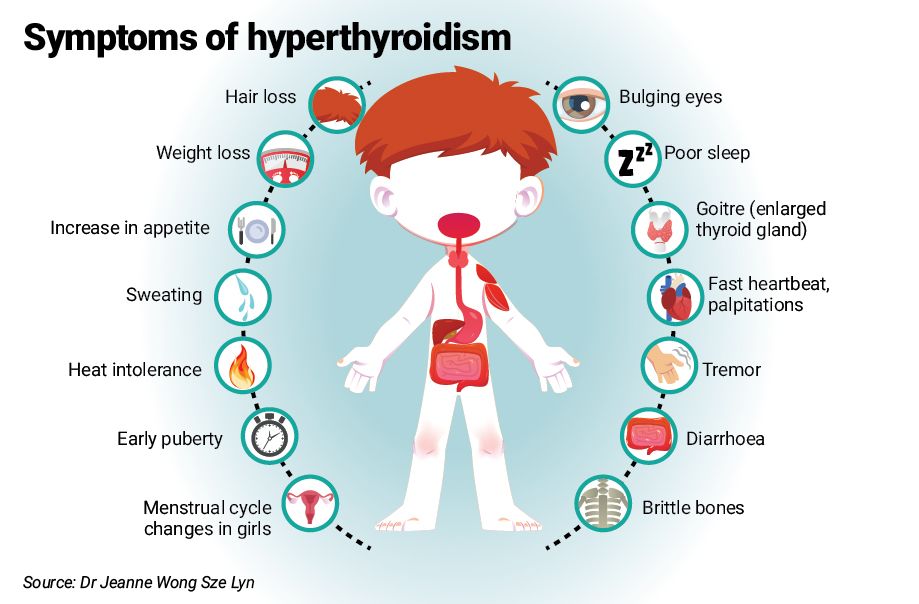
Among the most common signs and symptoms for hyperthyroidism are:
- Weight loss despite an increase in appetite
- Increased heartbeat or palpitations
- Heat intolerance
- Irritability
- Diarrhoea
- Tremors of hands and fingers
- Bulging eyes (exophthalmos), and
- Goitre.
Causes of hyperthyroidism
Hyperthyroidism is most commonly caused by two conditions.
This autoimmune disease is the most common cause of hyperthyroidism in both adults and children.
In Grave’s disease, the body produces thyroid antibodies that stimulate the thyroid gland to become overactive and produce excessive thyroid hormones.
Swelling of the thyroid gland, as well as swelling behind the eyes (exophthalmos) may occur.
Initial management consists of medical treatment to lower the production of thyroid hormones or block their action, and to relieve symptoms such as palpitations.
Babies born to mothers with thyroid disease are at risk of developing thyroid disorders and need to have their thyroid function monitored.
Depending on the mother’s thyroid disease and antibodies, the babies may develop either hyper- or hypothyroidism.
These conditions are often temporary and most babies will not need long-term treatment.
However, monitoring is needed until the child’s thyroid function is normalised.
Maternal Graves’ disease can lead to trans-placental transfer of maternal thyroid antibodies and cause thyrotoxicosis in the baby.
If a mother has current or previous history of Graves’ disease, both mother and baby must have their thyroid statuses evaluated in a timely manner.
Management of maternal hyperthyroidism during pregnancy is important because of the increased risk of miscarriage, preterm delivery and adverse effects on the baby’s thyroid function.
The importance of the small, butterfly-shaped thyroid gland is often overlooked, especially in children.
Increased awareness of thyroid disease in children allows for timely diagnosis and treatment, such as in the cases of baby Anne and Daniel.
Dr Jeanne Wong Sze Lyn is a consultant paediatrician and paediatric endocrinologist. This is the first article in a monthly series called Hormones and Kids. For more information, email starhealth@thestar.com.my. The information provided is for educational purposes only and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this column. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


