



The birth of a baby is a joyous occasion for parents.
The first question parents usually ask during prenatal hospital visits when ultrasound scans are performed, is: “Doctor, is my baby a boy or girl?’
There are occasions when, due to the position of the fetus, the doctor is unable to answer definitively, or the parents themselves may choose not to know and be “surprised” at the birth.
The vast majority of the time, it is quite clear from the genitalia after the baby is delivered whether the child is a boy or a girl.
However, for some babies born with ambiguous or atypical genitalia, the answer is not so clear.
Ambiguous genitalia is a condition in which a baby’s external genitals do not appear to be clearly male or female.
It is usually caused by a medical condition known as Differences of Sex Development (DSD), previously known as intersex.
Genes and appearance mismatch
DSD is a mismatch between a baby’s chromosomes or genetic material, and the appearance of their genitals.
It can happen for a number of reasons that can be related to differences in the development of the gonads (i.e. testes or ovaries), or hormonal signals that are responsible for the development of the genitalia during pregnancy.
Causes include genetics, unknown exposure to certain medications or hormones during pregnancy, or developmental problems in the baby during pregnancy, e.g. lack of blood flow to the testes or ovaries.
In some cases, the cause is unknown.
Up until eight weeks of a pregnancy, all babies develop in a similar way.
After that, the fetus in the mother’s womb develops gonads that can become a testes, an ovary or a variant.
A gonad is a term for both testes and ovaries.
There is one key gene that influences how the gonads develop.
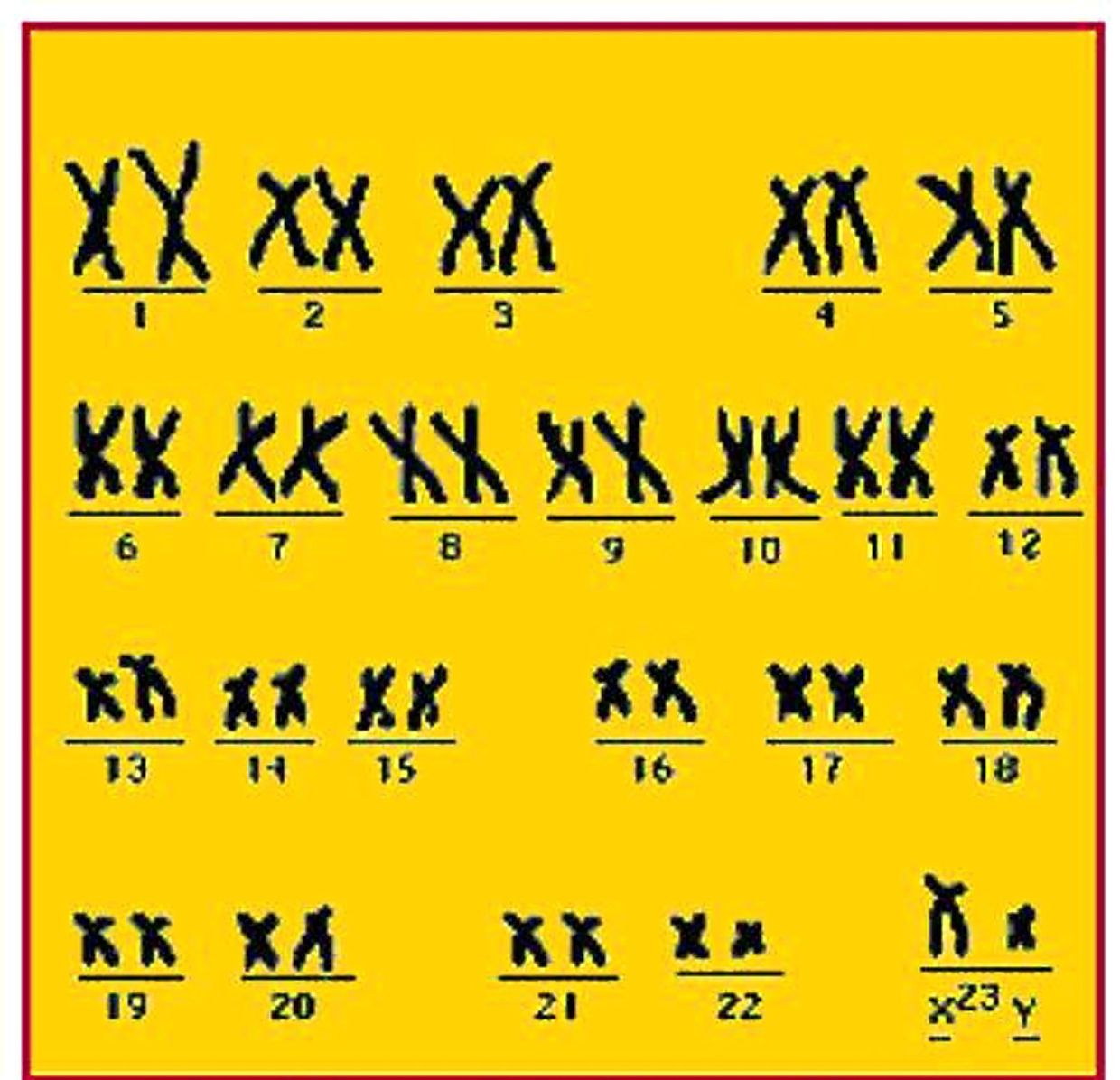
That gene is called the SRY gene.
The SRY gene is nearly always found on the Y chromosome.
It instructs the gonads to develop into testes.
If there is no Y chromosome, the baby’s gonads usually develop into ovaries.
The presence or absence of the SRY gene triggers a complex cascade of events involving numerous genes, enzymes and proteins working in a coordinated way.
The development of the gonads will determine what type of hormones are produced and how much.
If any of the processes described above are disrupted, then DSD or ambiguous genitalia will develop.
A child may present with DSD in infancy, childhood or adolescence.
Common types of DSD
Two common presentations of DSD are hypospadias and cliteromegaly.
Mild forms of hypospadias are as common as one in 300 boys worldwide.
Hypospadias is when a boy has his urethra (urinary opening) on the underside of the penis.
The severity of the condition is classified according to the distance of the urethra from its normal position at the tip of the penis.
Endocrine tests for underlying DSD are needed in severe hypospadias where the urinary opening is near the scrotum, or if it is associated with a small penis or an undescended testis.
Cliteromegaly is when a girl’s clitoris is larger than average; in severe cases, in may look like a penis.
The most common cause is classical congenital adrenal hyperplasia (CAH), which affects one in 28,000 girls worldwide.
In this condition, the girl is exposed to too much testosterone, resulting in an enlarged clitoris.
Tests must be urgently done to exclude CAH in baby girls who have a large clitoris.
This is as CAH is associated with a lack of other important hormones that regulate salt and blood pressure, which can result in life-threatening complications if not treated.
Another example of DSD is androgen insensitivity, which affects one in 40,000 babies.
This is when a baby who is genetically male is resistant to the effects of male hormones known as androgens.
Due to this, they may appear outwardly like a female.
Meanwhile, gonadal dysgenesis, which occurs in one in 100,000 babies, is when a baby of either sex experiences any congenital development disorder of their reproductive system.
In ovotesticular dysgenesis (previously known as hermaphroditism), which is a rare type of DSD, there is the presence of both testes and ovary tissues.
Symptoms and management
All babies with the following features should have further evaluation for an underlying DSD.
For an apparent female baby, the features include:
- An enlarged clitoris that looks like a small penis.
- An urethral opening positioned anywhere along, above or below the surface of the clitoris.
- Fused labia that may look like a scrotum.
- Swelling at the fused labia or at the groin, which may be testicular tissue.
For an apparent male baby, the features include:
- A small penis or micropenis (less than 2.5cm long) that looks like an enlarged clitoris.
- Severe hypospadias where the urethra is located near the scrotum.
- Hypospadias with any undescended testes.
The care of a child with DSD, depending on its severity, may involve a team of paediatricians who are further subspecialised in endocrinology, surgery, urology, psychology, psychiatry and genetics, as well as a gynaecologist.
Blood tests and ultrasound imaging to see the internal reproductive organs may be required.
Treatment includes surgery or hormone medications.
In some cases, no medical treatment is needed.
If it is not medically necessary, irreversible surgery to the genitalia should be postponed until the child is able to participate in decision-making and confirmation of their gender identity.

Gender identity
Gender identity is the identification of a person as a male or female.
It is influenced by genetics, exposure to hormones while still in the mother’s womb, and other factors that are not yet well understood.
For example, in a type of DSD known as complete androgen insensitivity syndrome (CAIS), the child has a Y chromosome typical for a male, but their body does not respond to the testosterone produced.
As such, they develop physically, and often identify, as a female.
In CAH, the child may show boyish behaviour, but most identify as female.
Most people with mild DSD identify with the gender that is consistent with their chromosomes, i.e. male if they have an X and a Y chromosome (XY), and female if they have two X chromosomes (XX).
However, in severe cases, assignment of the gender is challenging when the child is too young to clearly express a gender preference.
The parents and the medical team will work together based on available information to decide on the gender assignment of the baby.
However, in some cases, the child may feel differently once older and express a wish to change gender.
The impact of DSD or ambiguous genitalia on parents can be huge with feelings of confusion, guilt and fear of stigmatisation.
It is important that parents do not blame themselves.
Parents have no control over which genes are passed on to a baby or what can cause a DSD condition.
The best thing for a baby or child with DSD is to love and accept them as they are.
Dr Jeanne Wong Sze Lyn is a consultant paediatrician and paediatric endocrinologist. This is the third article in a monthly series called Hormones and Kids. For more information, email starhealth@thestar.com.my. The information provided is for educational purposes only and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this article. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


