



Osteoporosis is often associated with the elderly, but it can also affect children, particularly those who have medical conditions or lifestyle habits that increase their risk of this condition.
Left untreated, it can lead to fractures and bone deformities.
The word “osteoporosis” means “porous bones”.
It is a condition that causes weak and brittle bones.
The inside of healthy bone looks like a sponge.
This area of spongy bone is known as trabecular bone.
An outer shell of hard, dense bone, i.e. cortical bone, wraps around the trabecular bone.
In osteoporosis, the “holes” in trabecular bone grow larger and more numerous, while the cortical bone becomes thinner.
Out of balance
Bones are made of living tissue that are constantly growing and rebuilding.
From birth to young adulthood, we build more bone than we lose.
Around the age of 30, bone breakdown starts to occur faster than bone build-up, which causes a gradual loss of bone mass as we age.
Hence, the best time to maximise bone size and strength are during childhood, adolescence and early adulthood.
This is important to develop a strong skeleton that will support us throughout our life and lower the risk of osteoporosis.
In children with osteoporosis, not enough bone is built, or too much bone is lost.
The balance between the formation of new bone and breaking down of bone is influenced by:
- Age
- Genetic factors
- Hormones e.g. oestrogen and testosterone
- Physical activity
- The amount of calcium and vitamin D in your body.
Types of osteoporosis
There are different types of osteoporosis in children.
Primary osteoporosis is caused by genetic factors that cause an intrinsic defect in the bone, e.g. osteogenesis imperfecta.
Osteogenesis imperfecta is caused by a genetic mutation that affects the production of collagen, a protein that provides structure and strength to bones.
It affects both boys and girls with an incidence of 1:10,000-20,000 live births.
Secondary osteoporosis is caused by an underlying medical condition, nutritional deficiencies or medication.
Risk factors and secondary causes of osteoporosis include:
- Medical conditions, e.g. juvenile idiopathic arthritis, thalassaemia, kidney disease, hyperthyroidism, Cushing’s syndrome, inflammatory bowel disease, cystic fibrosis and diabetes.
- Medication, e.g. cancer treatments, prolonged use of corticosteroids (used to treat a wide range of conditions, including arthritis and respiratory diseases), and anti-convulsants (used to manage epilepsy).
- Poor nutrition (especially lack of calcium and vitamin D), resulting in underweight with poor muscle mass.
- Immobility, resulting in lack of weight- bearing activities that encourage bone density, e.g in children with cerebral palsy and neurological disabilities.
- Late (delayed) onset of puberty.
- Smoking and alcohol consumption.
Sometimes, no cause can be found and the disease is called idiopathic juvenile osteoporosis.
Easily broken
Osteoporosis is usually not diagnosed until after the child has broken a bone.
The fracture usually occurs following a minor fall or light bump.
In severe cases, it can occur during routine activities such as crawling, walking or running.
Common sites of fractures are the vertebrae (the bony segments of the spinal column), the thigh bone (femur) at the hip, and the wrist.
Fractures result in bone pain, deformities and difficulties with movement.
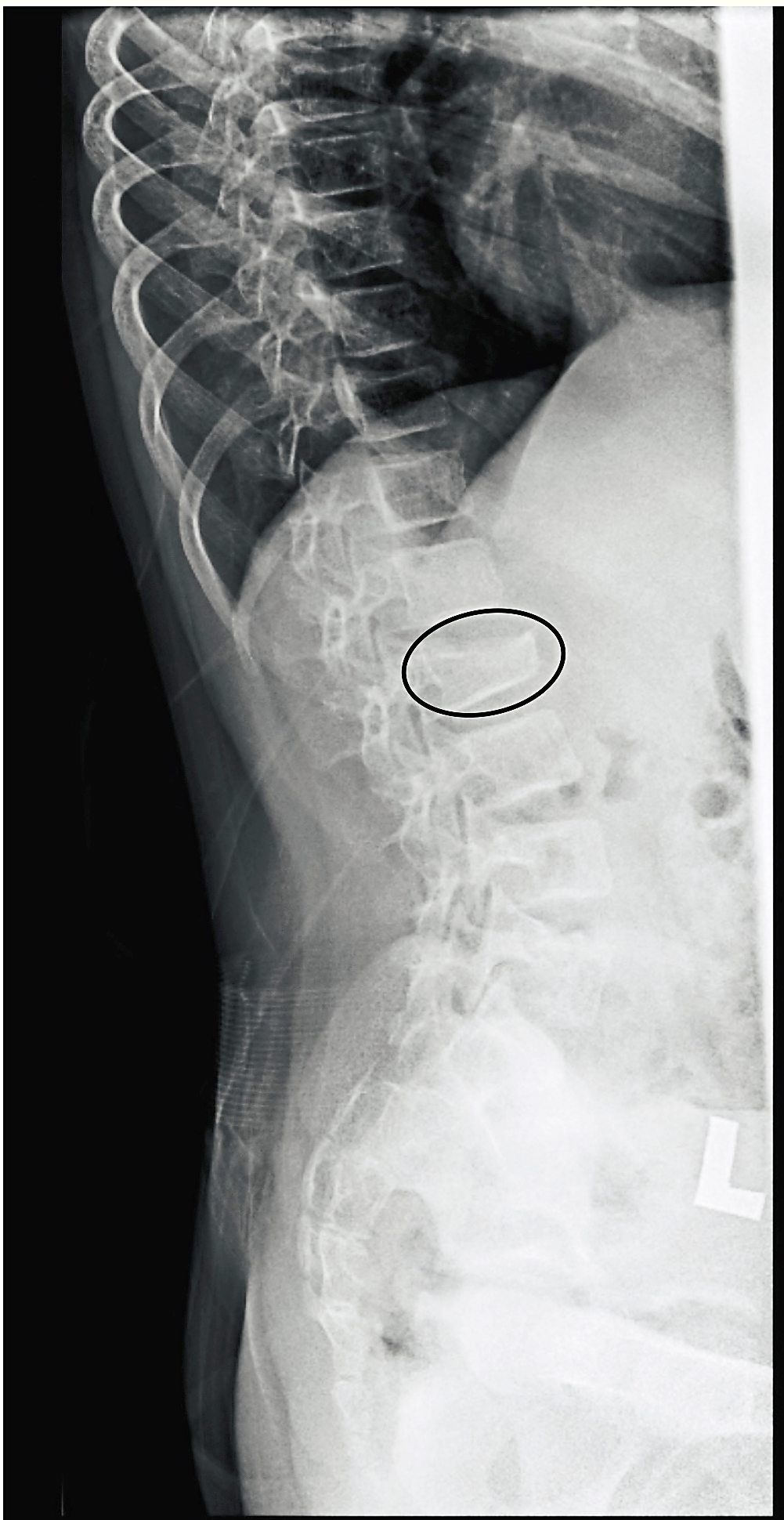
A fracture in the spine can occur because of compression of the weakened bone.
This type of fracture can lead to curving of the spine (scoliosis) with a loss of height.
Children with severe osteogenesis imperfecta may experience numerous fractures even before birth, while those with milder forms may have only a few fractures over their lifetime.
Children with osteogenesis imperfecta may also have a blue or gray tint to the white of the eyes (sclera), hearing loss and abnormal teeth.
Diagnosis and management
Diagnosis is based on medical and family history, physical examination, blood tests, radiographs and a bone densitometry scan known as a DEXA (or DXA) scan.
The diagnosis of osteoporosis is usually made by a history of vertebrae fractures or recurrent long bone fractures, together with evidence of low bone density.
It is important to note that the diagnosis in children should not be made solely based on the results of the DEXA scan.
The goals of the management of osteoporosis in children are:
- Treatment of the primary cause of the osteoporosis.
- Prevention of fractures, including vertebral fractures and scoliosis (curvature of the spine).
- Improvement in function, mobility and pain.
Treatment involves a combination of lifestyle changes, nutritional therapy and medications.
This may include changes to the child’s diet and exercise routine, medication to help strengthen bones, and physical therapy to improve balance and coordination.
Increasing calcium levels and ensuring adequate vitamin D intake are both essential in osteoporosis, which is where nutritional therapy comes in.
This type of therapy includes optimising the child’s weight and increasing the intake of foods that are high in calcium, vitamin D and other nutrients that promote bone health.
Vitamin D (cholecalciferol or ergocalciferol) and calcium supplements may be needed if the nutritional intake is inadequate.
Meanwhile, physical therapy is crucial to increase muscle mass and bone strength, with a focus on weight bearing, muscle strengthening, balance and flexibility.
Being active is very important, but it must be done in a safe manner with input from a physiotherapist.
High-impact exercises that exert high stress on the joints, lifting of heavy objects, and excessive bending or twisting of the spine, should be avoided in severe osteoporosis.
In some cases, surgical intervention may be necessary to correct bone deformities to assist in movement.
In cases where the child has recurrent long bone fractures or any vertebrae fractures, special medications called bisphosphonates are beneficial to improve bone density and prevent further fractures.
For example, infants with severe osteogenesis imperfecta will benefit from early intravenous bisphosphonates to minimise further fractures and improve quality of life.
Bisphosphonates require monitoring for side effects, but their benefits in severe osteoporosis often outweigh any potential side effects.
Another important management goal is to ensure that the child has a normal onset of puberty.
Preventive measures
It is important for children at risk of developing osteoporosis to be regularly monitored by a healthcare team.
They must also be sure to have adequate nutrition, particularly calcium and vitamin D, and exercise or be physically active on a regular basis, especially when it comes to weight-bearing activities.
Adolescents should also avoid smoking and alcohol.
Any risk factors or underlying conditions they might have should also be properly managed.
In conclusion, osteoporosis can occur in children and adolescents, not just older adults.
It is a serious bone condition that can have lifelong consequences.
Awareness among healthcare professionals and parents is essential.
By recognising the risk factors, prevention may be possible.
Recognition of symptoms enables early treatment to achieve the best possible outcomes for the child’s long-term health and well-being.
Dr Jeanne Wong Sze Lyn is a consultant paediatrician and paediatric endocrinologist. This is the fifth article in a monthly series called Hormones and Kids. For more information, email starhealth@thestar.com.my. The information provided is for educational purposes only and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this column. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


