Thyroid cancer is the eigth most common cancer amongst females in Malaysia with the incidence of 3.8 per 100,000-population.
While this cancer is definitely not as common as breast cancer, public awareness of this disease remains poor.
Most people will learn about the cancer only when someone they know or they themselves are diagnosed with it.
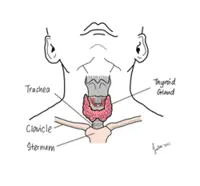
The thyroid gland is an important organ in the shape of a butterfly located at the anterior aspect of the neck.
It is usually not visualised unless enlarged.
The hormones that it produces serves like a traffic light and coordinates the bodily functions.
If there is over production of the thyroid hormones (hyperthyroidism), one will experience palpitations, anxiety, heat intolerance and various conditions.
On the contrary, if there is reduce production of the thyroid hormones (hypothyroidism), one will experience lethargy, brain fog, weight gain, intolerance to cold, etc.
Cancer refers to abnormal growth of cells within an organ that is capable of infiltrating, damaging normal body tissue and spreading throughout the body.
Thus, thyroid cancer occurs when the thyroid tissues turn “bad” and starts growing abnormally.
Most of the thyroid cancers tend to be slow-growing and are often detected incidentally during health screening or when the cancer has grown to a noticeable size.
Most thyroid cancers occur spontaneously with no identifiable cause.
A minority of patients have familial mutations that are passed on through the generations such as multiple endocrine neoplasia (MEN) type 2, familial adenomatous polyposis (FAP) and hamartoma tumour syndrome.
Sometimes, patients who had radiotherapy to the neck for other cancers at a younger age might also develop thyroid cancer when they are older.
Thyroid cancer occurs more in women, and the reason remains unknown.
No. There are many types of thyroid cancers and the treatment varies according to the type of cancer.
Nonetheless, the most frequently encountered thyroid cancers are the well-differentiated ones i.e. they are “matured thyroid tissues” that turn “bad”.
These includes predominantly the papillary thyroid cancer subtype (80-85% of all thyroid cancer cases) and follicular thyroid cancer subtype (five to 10% of all thyroid cancer cases).
Most thyroid cancers are insidious and are detected during health screening.
Some patients present with neck swellings, and rarely with dysphagia (difficulty swallowing) and hoarseness of voice.
In cases of aggressive thyroid cancer, patients may present with acutely enlarging neck swelling, shortness of breath or bone fracture.
Neck swelling can be due to various causes such as lymphadenitis (infected lymph nodes), lymphoma (cancer of the lymph nodes) or even metastases from other cancer.
Ultrasound of the neck is usually performed and based on the findings, the attending doctor will decide if any tissue sampling is needed.
In most instances, a simple fine-needle aspiration of the lesion will suffice.
Uncommonly, the doctor will recommend removing the affected thyroid lobe for evaluation.
As in any cancer, surgical removal of the tumour will be the ideal.
However, this would again depend if the cancer is resectable or there is a need for pre-surgical therapy to reduce the bulk of the tumour.
In the case of thyroid cancer and depending on the risk category, total thyroidectomy is usually performed.
Thyroid lobectomy will only be performed for low-risk cases.
Following surgery and depending on the examination of the removed tissues, doctors will then decide on the next step of management.
Well-differentiated thyroid cancers, as the commonest thyroid cancer, are treated with thyroxine suppression therapy and radioiodine-131 unless the cancer becomes refractory.
Other thyroid cancers are treated with chemo- and radiotherapies.
It’s basically a radioactive form of iodine which is used to destroy thyroid cells including thyroid cancers.
This is a targeted therapy where the radioiodine-131 is ingested and once absorbed, will be taken up by cells utilising iodine – which is the thyroid cells.
Well-differentiated thyroid cancers behave similar to thyroid cells and will take-up radioiodine-131 though less avidly.
Once within the normal or thyroid cancer cells, the radiation from the radiodine-131 will cause cell-damage and cell-death.
Doctors will decide on the radioiodine-131 (measured in miliCuries) dosage to be given depending on the risk stratification.
Patients would only need to ingest radioiodine-131 once in a period not less than three months during each course of therapy.
Radiation-isolation is only required until permissible levels for release to the public is achieved.
Unlike radiotherapy where radiation is administered in multiple fractions (doses) to cause cell-death, radioiodine-131 is only administered once and will continue to cause damage and cell-death in the thyroid cells in a reducing exponential level for a period of three months.
Pre-therapy preparations are also important to ensure the best outcome e.g. low iodine-diet and thyroxine withdrawal or injection of recombinant human thyroid stimulating hormone (TSH).
Radioiodine-131 has theranostic (acronym for therapy and diagnostic) properties whereby it allows doctors to treat and image the distribution of the thyroid cells in body.
Radioidoine-131 is safe and has been used since 1940’s.
The intended dose of radiation is essentially restricted to the thyroid tissues.
This is similar to radiotherapy where external beam radiation is delivered to the tissue of interest with the intended site receiving the most radiation and the tissue lying in the path of the radiation receiving lower doses.
Contrastingly, the type of radiation in radioiodine-131 therapy is different and the effect of the radiation is basically very limited particularly to the tissues surrounding the targeted site.
Importantly, the remaining radioiodine-131 which is not taken up by the targeted thyroid tissue is excreted in the urine.
Thus, the radiation exposure to patients from radioiodine-131 therapy is certainly insignificant compared to the radiation exposure from nuclear bombs or nuclear power-plant meltdown.
For patients who had thyroid surgery to remove the entire thyroid gland, their bodies lack thyroid hormones and so, they require hormonal (thyroxine) replacement.
Unlike normal patients with insufficient thyroid hormone, thyroid cancer patients will require relatively higher doses to suppress the pituitary gland from stimulating the possible residual thyroid cells.
This suppression will be gradually tapered to an appropriate level accordingly by the attending doctor.
Most well-differentiated thyroid cancer patients, especially younger patients, have good prognosis.
The disease-specific 10-year survival for stage one thyroid cancer is excellent with expected survival of 98-100%.
Unfortunately, the same cannot be said for anaplastic thyroid cancer, which is rare but the most aggressive one; it has a one-year survival of approximately 20%.
Family members of patients with well-differentiated thyroid cancer are advised to have careful history and directed neck examination as part of their routine health maintenance.
Those without history but presenting with suspicious neck lesions or symptoms of unexplained hoarseness of voice or difficulty swallowing should seek medical attention quickly.
Essentially, early and optimal treatment makes the difference.
Dr Alex Khoo Cheen Hoe is a consultant nuclear medicine physician. For more information, email starhealth@thestar.com.my. The information provided is for educational and communication purposes only, and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this article. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.