



What is the most complex organ in the human body?
Undoubtedly, most of us will think of the brain.
Powered by energy-rich glucose and oxygen through the blood circulatory system, the brain is one of the biggest and most complex organs in our body.
This amazing organ, physically soft with a spongy mixture of protein and fat, weighs only approximately 2% of our total body weight, but utilises about a fifth of our energy!
The brain is composed of more than a hundred billion brain cells, which are made up of neurons and glia that communicate in trillions of connections known as synapses.
These unique neurons are nerve cells that conduct electrical impulses.
Meanwhile, glia cells provide structural protection and nutritional support for the neurons.
The brain is particularly vulnerable to toxic exposure and hypoxic conditions (i.e. low levels of oxygen).
Hence, the brain is shielded from an influx of harmful substances by a layer of tight-packed specialised endothelial cells known as the blood-brain barrier.
This barrier provides a natural protective function to impede the entry of harmful substances from the peripheral blood circulation into the central nervous system (CNS).
It is composed of different cell types, such as astrocytes, pericytes, endothelial cells, neurons and microglial cells.
All these cells play important and interconnecting roles in regulating the function of the brain.
The passage of molecules or ions through the blood-brain barrier is tightly regulated by cellular transporters and carriers.
This allows the delivery of nutrients into the brain, removal of unwanted toxins, and recruitment of leukocytes (white blood cells) or other immune system molecules necessary to maintain normal brain homeostasis.
The integrity of the barrier can be altered by the onset of disease.
Neuroinflammation in an ischaemic stroke (where there’s blockage of a blood vessel supplying the brain), systemic infection and inflammation, inflammatory bowel disease and hypertensive encephalopathy are some examples of causes linked to a breakdown of the blood-brain barrier.
It is also a natural phenomenon correlated with ageing, initially occurring at the hippocampus situated at the medial temporal lobe, which is essential for episodic and spatial memory.
A link to three conditions
Epilepsy is a chronic CNS disorder characterised by recurrent seizures.
According to a study conducted by local researchers, the frequency of epilepsy was found to be higher in males.
Meanwhile, lifetime frequency, i.e. the frequency of epilepsy at any point of life in the population concerned (in this case, Malaysia) was estimated at 7.8 per 1,000 persons.
One in five patients with epilepsy in Malaysia died from the condition.
This implies the importance of treatments and access to adequate and appropriate treatment and care.
Increased blood-brain barrier permeability due to a “leaky” vasculature has been identified as the common underlying cause for epilepsy, Alzheimer’s disease and Parkinson’s disease.
There is also a growing body of evidence supporting the theory that seizures can promote amyloid-beta peptide and tau protein deposits, which can then lead to neurodegenerative processes that result in conditions like Alzheimer’s and Parkinson’s.
In two separate studies, it was reported that Alzheimer’s disease occurs six times more often in patients with epilepsy, and that seizures are highly repetitive and also occur in patients with dementia from Alzheimer’s.
A study done in the United Kingdom found that “people with epilepsy are 2.5 times more likely to be diagnosed with Parkinson’s disease than the general population”.
Nanoparticles for transport
An avalanche of research has centred on less or non-invasive methods to avoid some of the side effects associated with intrathecal administration of treatments into the spinal cord.
An intrathecal injection is where the drug is injected into the spinal cord fluid via a lumbar puncture.
Some of the side effects of this procedure include bleeding in the brain (haemorrhage), infection and and swelling of the brain (oedema).
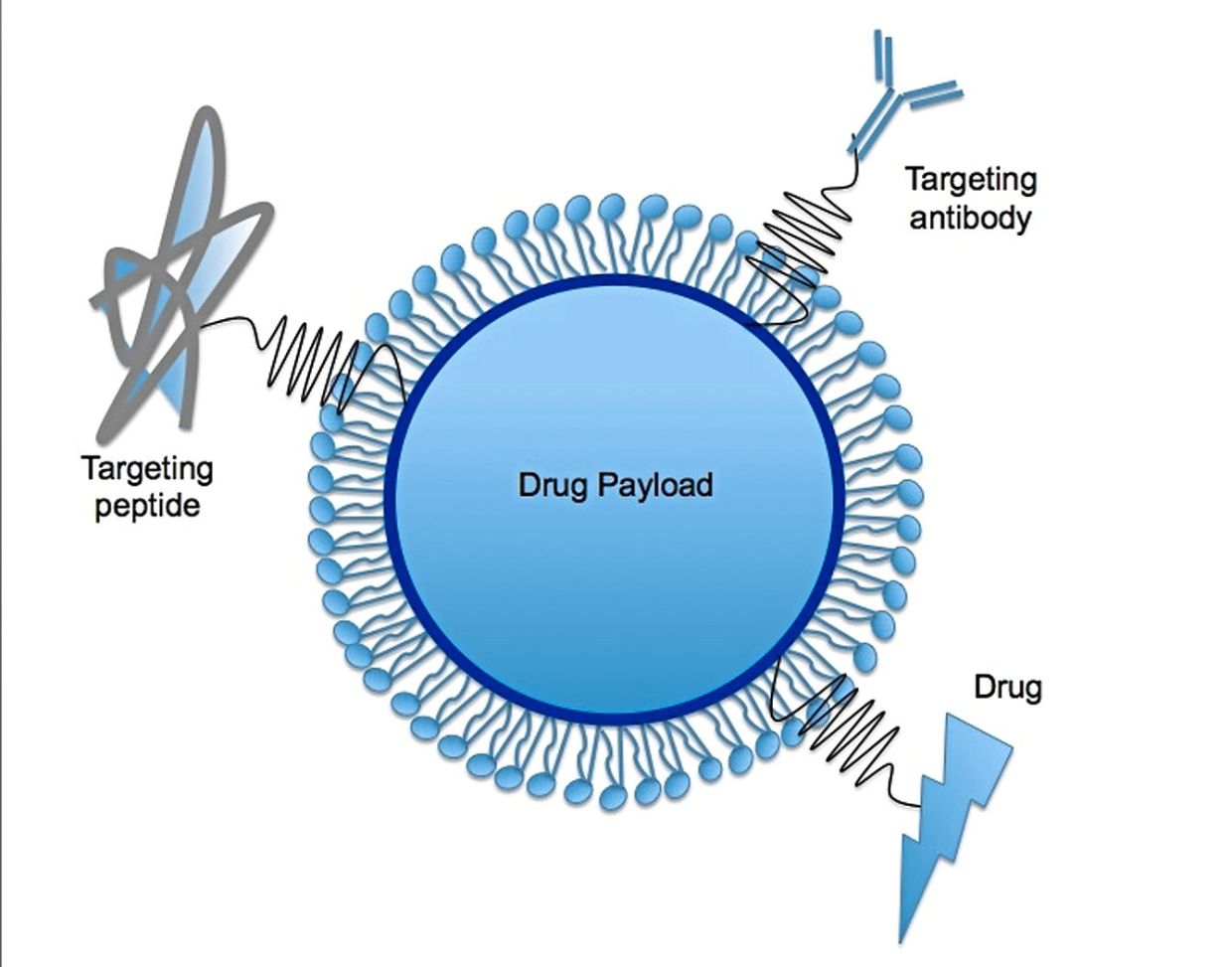
In particular, there has been a growing interest in the use of nanoparticles to traverse through the blood-brain barrier, owing to their very small size, i.e. about 100 times smaller than a strand of human hair in diameter.
Nanoparticles can be designed with different shapes and sizes (within the nanometre range), as well as with desired properties (e.g. biodegradability) to meet the current demands in the production of functional materials.
They have widespread applications; however, the most commonly-known uses are in the cosmetics, food manufacturing and biomedical industries.
In 1995, cancer drug doxorubicin was the firstever nano-based product to be granted approval by the US Food and Drug Administration (FDA).
The number of nanotechnology products entering clinical trials since then have only grown larger.
As one of the approaches widely studied to facilitate the transport of medicinal compounds across the blood-brain barrier, the use of nanoparticles is especially promising as its mechanism does not affect the baseline permeability of the barrier.
Another fascinating approach involves the engineering of the protein corona, red blood cells and extracellular vesicles as nanoparticles bearing naturally-occurring components to cross the blood-brain barrier.
Nanoparticles made with this strategy have “stealth-like” properties as they can evade recognition and sequestration (and removal) by the immune system.
Importantly, this allows the nanoparticles to escape destruction in the event of an inflammatory response.
Crossing the barrier
In the case of epilepsy, Alzheimer’s disease and Parkinson’s disease, encouraging findings have been obtained with a host of nanoparticle strategies, especially with the versatility to accommodate more than one function into the nanoparticle design.
Nanoparticles have been engineered to effectively transport drugs across the blood-brain barrier by targeting receptors involved in endocytosis.
Endocytosis is a process by which a cell brings substances into itself.
The external substance is surrounded by a part of the cell’s membrane, which then breaks off to form a sphere with the substance within it, known as a vacuole.
For this process to occur, the external substance and cell membrane need to be able to “lock” onto one another.
One common way this occurs is when the substance has a ligand that matches with a receptor on the cell membrane, similar to a key and lock.
When the ligand (a molecule or atom) combines with the receptor (a protein molecule), its shape will be changed and this will trigger the endocytic process.
For this approach, the surfaces of the nanoparticles are modified with the appropriate ligands.
A wide range of ligands have been explored by researchers.
Examples include lectin, cardiolipin and heparin surface-decorated nanoparticles for Parkinson’s disease, and lactoferrin, apolipoprotein-E, transferrin and thiolated OX26 for epilepsy, Alzheimer’s disease, as well as Parkinson’s.
Research has also shown that adding in a scaffold of bispecific antibodies, i.e. anti-transferrin receptor and anti-beta secretase, reduces amyloid-beta peptide deposits in the cerebrospinal fluid and brain tissues of cynomolgus monkeys that received the intravenous (IV) injections.
Delivering potential treatments

Nanoparticles might also have the potential to target key mechanisms that fundamentally contribute to the three neurological disorders.
For example, an animal study using rats, described the delivery of an anti-epileptic peptide, galanin, that is capable of inhibiting glutamate release in the hippocampus.
An increase in glutamate, a neurotransmitter, is associated with the onset of seizures.
Other studies have targeted the alpha-synuclein protein, which plays a role in Parkinson’s disease.
It is thought that there is a misfolding of this protein in people with Parkinson’s, causing the proteins to clump together to form Lewy Bodies.
These clumps are theorised to be toxic and spread the disease throughout the brain as they get passed from one neuron to the other.
One animal study using mice, assessed the inhibition of alpha-synuclein fibrillisation and protection from the progressive loss of dopaminergic neurons.
The formation of fibrils by the alpha-synuclein protein contributes to its toxicity, while dopamine, a neurotransmitter, is low in Parkinson’s disease.
In another approach, researchers have proven that alpha-synuclein can be prevented from activating in microglial cells via scavenger receptor CD36-binding nanoparticles.
The CD36 receptor is a glycoprotein found in cells in the blood-brain barrier, such as astrocytes and microglia.
Another strategy uses glial cell-derived neurotrophic factor (GDNF), which is a key protein in regulating the survival and differentiation of brain cells that produce dopamine.
In a rat model of Parkinson’s disease, lipid nanocarriers loaded with GDNF plasmids were combined with microbubbles for MRI-guided focused ultrasound-mediated effects that led to a reduction in nerve cell death and helped alleviate behavioural changes due to the disease.
A plasmid is a small DNA molecule within a cell, which is separate from chromosomal DNA and can replicate by itself.
Another method of delivery using GDNF retrovirus-loaded microbubbles and focused ultrasound also proved successful in delivering the GDNF retrovirus into nerve cells.
Alternatively, the nose-to-brain route of administration (rather than the conventional IV infusion or injection) could be a way to improve the delivery of drug-loaded and/or targeted nanoparticles to specific regions of the brain.
Delivery via this route bypasses the blood-brain barrier and enables direct delivery to the brain along the olfactory and trigeminal nerves.
This strategy, however, requires the nanoparticles to have augmented properties, such as protecting the molecules within them from being destroyed or damaged in the nasal cavity, and getting through the nose’s mucosal barrier.
More to come
A plethora of research on nanoparticles for disease treatment can be expected in the forthcoming years.
This includes clinical trials that can evaluate the potential short- and long-term adverse effects that may be triggered by their administration and uptake in the human body.
Although the journey towards clinical translation (i.e. nanoparticles approved for brain targeting and treatment) may be arduous as it requires substantial time and effort, there remains a light at the end of the tunnel for novel and tailored therapies to be developed in the near future to treat neurological disorders and injuries of the nervous system, in what may be known as the ‘precision medicine’ approach.
Dr Lee Tze Yan is a senior lecturer for Molecular Medicine at the Perdana University School of Liberal Arts, Science and Technology. Loo Yan Shan is a PhD student in Nanomedicine at Universiti Putra Malaysia. For more information, email starhealth@thestar.com.my. The information provided is for educational and communication purposes only, and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this article. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


