



One of the most devastating things that can happen to a parent is finding out that your child has an incurable, terminal illness.
The signs that Branden Lim, 12, was not a regular healthy baby came as soon as he was born.
According to mother Yap Sook Yee, 48, her younger son had to be rushed to the neonatal intensive care unit (NICU) immediately after delivery as he couldn’t really cry due to having fluid in his lungs.
After spending his first eight days of life in the hospital, Branden fortunately recovered and was able to go home.
Three months passed uneventfully, with Branden achieving the milestone of turning over by himself – but as Yap shares, that was “the first and last time he ever did it”.
From then on, he started missing more and more growth milestones, such as sitting up and crawling.
While Yap and husband Edmund Lim, 49, brought him to see a number of paediatricians and interventions like physiotherapy were prescribed, it wasn’t until Branden only gained 100g between six months and one year of age that the alarm bells really started ringing in earnest.
Feeling that something was really not right, Yap did some research on her own into the possible conditions that might be affecting her child.
Armed with a few possibilities, she brought Branden to his paediatrician to discuss them.
The doctor agreed that her son might indeed have an undiagnosed condition and referred them to a paediatric geneticist for further consultation.
After doing multiple tests, it was confirmed that Branden had the rare disease known as spinal muscular atrophy (SMA).
This genetic condition occurs when a child inherits two defective copies of the recessive SMN1 gene – one from each carrier parent.
The SMN1 gene is in charge of producing a protein called survival motor neuron (SMN), which, as its name states, is crucial for the survival of motor neurons.
Motor neurons are nerve cells located within the central nervous system, which control both voluntary and involuntary muscle movement.
The lack of the SMN protein leads to the early death of these motor neurons.
As these cells have very limited regeneration capacities, this has a very serious impact on all the functions of the body that require muscle movement.
This not only includes movement like turning over, sitting up and crawling, but also essential functions like swallowing and breathing.
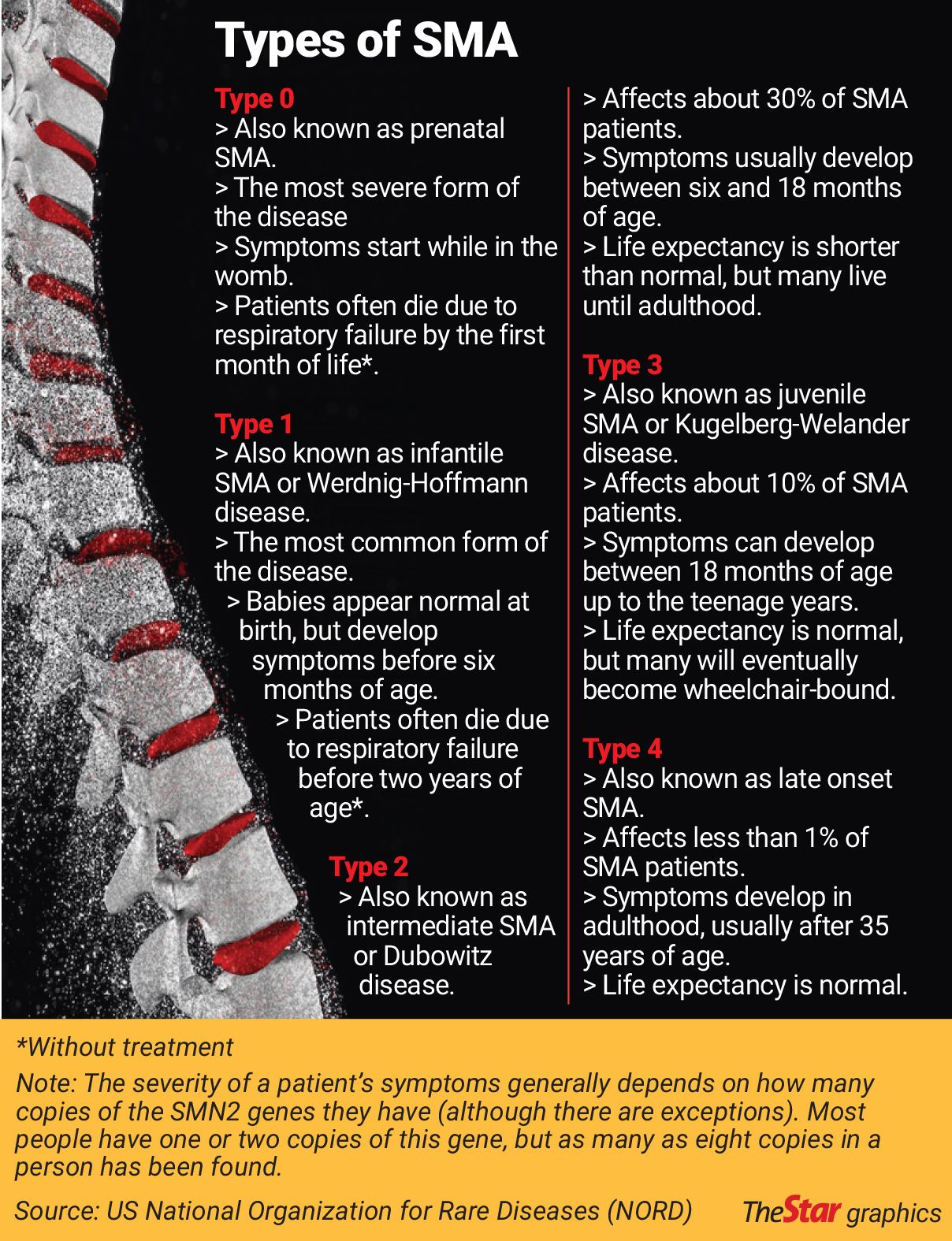
There are five types of SMA, which are classified according to when the symptoms first develop, and subsequently, how severe the disease will be (see graphic below).
Branden was diagnosed to have SMA type 1 – the most common and second most severe type.
Striving for survival
Yap initially did not tell Lim about Branden’s tests as he was working in London on an overseas assignment at that time.
However, the then-commercial manager returned in time for them to receive the test results together.
“It was like the whole house had fallen down around us; we were totally shocked by the diagnosis,” he recalls.
Their shock and grief were compounded by the fact that the paediatric geneticist essentially told them there was nothing they could do for their son.
With no cure or treatment for SMA at that time, type 1 patients typically had a life expectancy of two years or less.
But neither Yap nor Lim are the types to take things lying down; they immediately started researching the condition.
They quickly discovered and signed up with Families of SMA, which sent them a care package on SMA.
This US-based non-profit was formed by parents of children with SMA, which aims to support families affected by the condition, and to fund research into treatments for it.
Their immediate focus was to manage Branden’s symptoms and enable him to have the best possible quality of life.
“When Branden was diagnosed, of course at that point in time, we were mostly distracted with trying to figure out how we could care for him first, because we had so many regular issues that were often life-threatening.
“But before long, as we were looking at sources of information around the world, the research pipeline was clearly there,” Lim says.
“The research pipeline is very clear to show us where drug therapies were being developed, how they were intended to work, and what stage they were at.
“So when you have that pipeline, you can see it coming through, you just don’t know when because it can fail during clinical trials.”
He shares that a couple of years after Branden’s diagnosis, they started engaging with the pharmaceutical companies that were involved in developing drugs for SMA.
That’s when they started learning more about clinical trials.
Clinical trials abroad

“Now, clinical trials are about being a ‘guinea pig’, but I guess when you look at it from our situation, if we didn’t take the chance, we know where things would end up anyway – which would be a pretty unhappy ending sooner than we would like.
“And because SMA is progressive, you’re not at the same stage all the time, you’re continuously losing function,” Lim says.
You have to “take the bet”, as Yap says.
However, with all the trials being done overseas, the question was how to access them from Malaysia?
Lim shares: “I used LinkedIn to track down people in (the) pharma(ceutical industry) to try to figure out how things work.
“Unfortunately, we didn’t have a lot of guidance; it took us a bit of time to understand that it wasn’t pharma’s decision, it was the doctor’s decision.”
Doctors, whether in university, public or private hospitals, are the ones responsible for enrolling patients who meet the appropriate criteria into clinical trials.
The problem then arose as to how to enable Branden to become a patient of an overseas doctor involved in one of the trials, as this is a prerequisite for enrollment.
Moving to the country the clinical trial was taking place in was an option, but things never fell into place properly for it to be a real choice, according to Lim.
As SMA is a rare disease, and thus, has a smaller pool of patients willing and able to participate in clinical trials, some doctors might be willing to enrol patients based overseas.
However, there are also other issues involved.
“Even if the doctor is willing to enrol you, you have a whole host of other issues – regulatory, compliance, all these sort of things.
“But we made the effort to go through it, to fully understand the process, which is difficult, but not impossible,” Lim says.
He adds that while they have seen cases where patients have been enrolled from overseas, both the pharmaceutical company and the doctor(s) involved have to be willing to facilitate the process.
“Unfortunately, the timing never worked out for Branden,” he says.
For example, Lim got in touch with AveXis, a US-based biotechnology company that was developing a genetic therapy to treat SMA, via LinkedIn.
“One of their senior reps was willing to have a conversation with us on the phone, and Sook Yee subsequently met them at the 2016 World Orphan Drug Congress,” he says.
And while they learnt that there was a real possibility for international recruitment for SMA clinical trials, Branden, who was six years old then, was already too old to join the one for the genetic therapy named onasemnogene abeparvovec-xioi.
This drug is a one-time treatment, which was approved by the US Food and Drug Administration (FDA) in May 2019 for children less than two years old.
It replaces one of the patient’s defective SMN1 genes with a new, working copy.
AveXis was bought by Swiss-American pharmaceutical corporation Novartis in 2018 and renamed Novartis Gene Therapies.
Compassionate treatment
In June 2016, Yap and Lim founded WeCareJourney, a non-profit organisation that helps provide resources and support for Malaysian patients with SMA and their families, raises awareness about SMA, and engages with various stakeholders to help facilitate access to treatments for SMA for both Malaysian and Asean patients.
Lim resigned from his corporate job to go full-time into SMA activism, while Yap gave up her plans to eventually return to the workforce after her sons were a bit older, to do the same.
It was in his capacity as WeCareJourney president that Lim was invited by Swiss healthcare company Roche to attend the 2019 International Experience Exchange with Patient Organizations (IEEPO).
He was given the opportunity to ask Roche chief executive officer Severin Schwan a question directly on stage in front of the audience.
“So, of course, the question I had for him was around unmet needs for SMA patients in countries like Malaysia, which were, at the time, thought secondary to the developed nations.
“So my question was, how is this fair? What can we do to enable more equitable access around the world?” Lim shares.
Although he is unsure whether or not this interaction made a difference, he notes that Roche appeared to soon start considering their SMA drug access in countries that were probably not originally on their priority list, like Malaysia, Singapore and Thailand.
Roche, through its independent subsidiary Genentech, markets the SMA drug risdiplam.
It is the first oral drug to be approved by the US FDA for SMA, and can be taken by patients from birth up to 60 years of age.
It helps the SMN2 gene make more functional versions of the SMN protein, and is a lifelong treatment.
The SMN2 genes are typically unaffected by SMA, but they produce far less functional protein compared to normal SMN1 genes.
In July 2020, Roche introduced the expanded access programme for risdiplam in Malaysia.
This programme allowed SMA patients who otherwise had no access to approved treatments or those in clinical trials, to obtain risdiplam for free under compassionate use.
Branden was one of the fortunate patients who managed to get into the programme, and is now being treated with risdiplam.
However, Lim says that the programme is no longer accepting new patients as the drug is now available commercially in Malaysia.
It was approved for children aged two months and older up to adults aged 60 by the US FDA in August 2020, and for children aged below two months last May.
Lim gives credit to the National Pharmaceutical Regulatory Agency (NPRA) for being accommodating enough to grant Import Permits for the then-unregistered drug through its Application to Import Product for the Treatment of Life-Threatening Illnesses pathway on an individual, named patient basis.
According to Health Ministry Pharmaceutical Services senior director Norhaliza A Halim, this pathway ensures continuous access to medicines needed for the treatment of a patient in cases where there are no registered or suitable medicines or treatment options available locally.
But there is a end date stipulated for the expanded access programme and its provision of free treatment.
“It is hanging over Branden’s head and the head of all these other children.
“Reassurances are given (that the free treatment will be continued), but reassurances are just that,” Lim says matter-of-factly.

Patient access programmes
All the knowledge and connections that Yap and Lim have gained in their own journey is also being utilised for Malaysian patients with SMA through their non-profit organisation.
For example, WeCareJourney signed a Memorandum of Understanding (MoU) with healthcare access company Axios International last May (2022) to collaborate on a patient access programme for nusinersen.
Marketed by US biotechnology company Biogen, this drug was the firstever SMA treatment approved by the US FDA in December 2016.
Similar to risdiplam, nusinersen works by boosting the production of functional SMN proteins by the SMN2 gene and can be given to infants up to the elderly.
It needs to be injected into the cerebrospinal fluid of the spinal cord via an intrathecal injection.
After an initial four loading doses, the drug is administered once every four months for the rest of the patient’s life.
Through this partnership, WeCareJourney will help to identify SMA patients who could benefit from the programme, which requires some amount of co-pay by the patient.
Axios will evaluate each patient and coordinate between Biogen and the hospital for drug delivery (see this Sunday’s article in StarHealth for more information).
Lim shares: “One of the frustrations in our early days was always one party saying something’s not ready, waiting for the other party.
“So that drove a lot of the effort that we put in in the early days – to make all these connections and to have all these conversations.
“Because who else is more motivated to do it than the parents of a child who is facing a traumatic, life-limiting condition?”
This article is part of the second package of a short series written as part of the US National Press Foundation’s 2022 Covering Rare Diseases: Journalism Fellowship & Global Reporting Grant. The next one will be published this Sunday (Jan 8, 2023) in StarHealth.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


