



Lung nodules – small round growths in the lungs – are common findings in imaging tests.
They are often detected by chance during a routine medical check-up, a vehicle accident or while screening for a different condition.
Due to their small size, they rarely cause any symptoms such as pain or breathing problems, so their appearance is not always something to worry about.
Lung nodules are usually caused by scar tissue, a healed infection that you may not have known of, inflammation or some irritant in the air.
However, because some nodules can be early signs of lung cancer, all nodules require medical evaluation to determine the underlying cause and the need for further monitoring or intervention.
The seriousness depends on factors like the nodule’s size, growth rate and appearance.
Another way the nodule is picked up is when the doctor orders a computed tomography (CT) scan, after a patient reports respiratory issues such as a persistent cough, recurrent chest infection or unexplained weight loss, among others.
Senior cardiothoracic surgeon Professor Dr Anand Sachithanandan says in the majority of the cases, nodules are probably benign, but to ascertain that, patient surveillance is required.
“But we do clinical risk profiling – we want to know their age, family history, cancer history, gender, ethnicity, are they a smoker, etc – and we look at the features of the nodule.
“Based on those information, we then decide on the next step,” he says.
Lung diseases in Malaysia are a leading cause of both hospitalisations and deaths, with respiratory ailments accounting for the second highest rate of hospital admissions and mortality in public hospitals in 2022.
According to the Malaysian Cancer Registry Report for 2017-2021, lung cancer is the second most common cancer among men and the third most prevalent among women.
Alarmingly, a vast majority of those diagnosed with lung cancer – 76% of men and 94% of women – are only identified at advanced stages (Stage 3 and 4), severely limiting their treatment options and chances of survival.
Public awareness plays a vital role for timely medical consultations to improve patient outcome, and during November’s Lung Cancer Awareness Month, campaigns and programmes continue to highlight the importance of early diagnosis and treatment.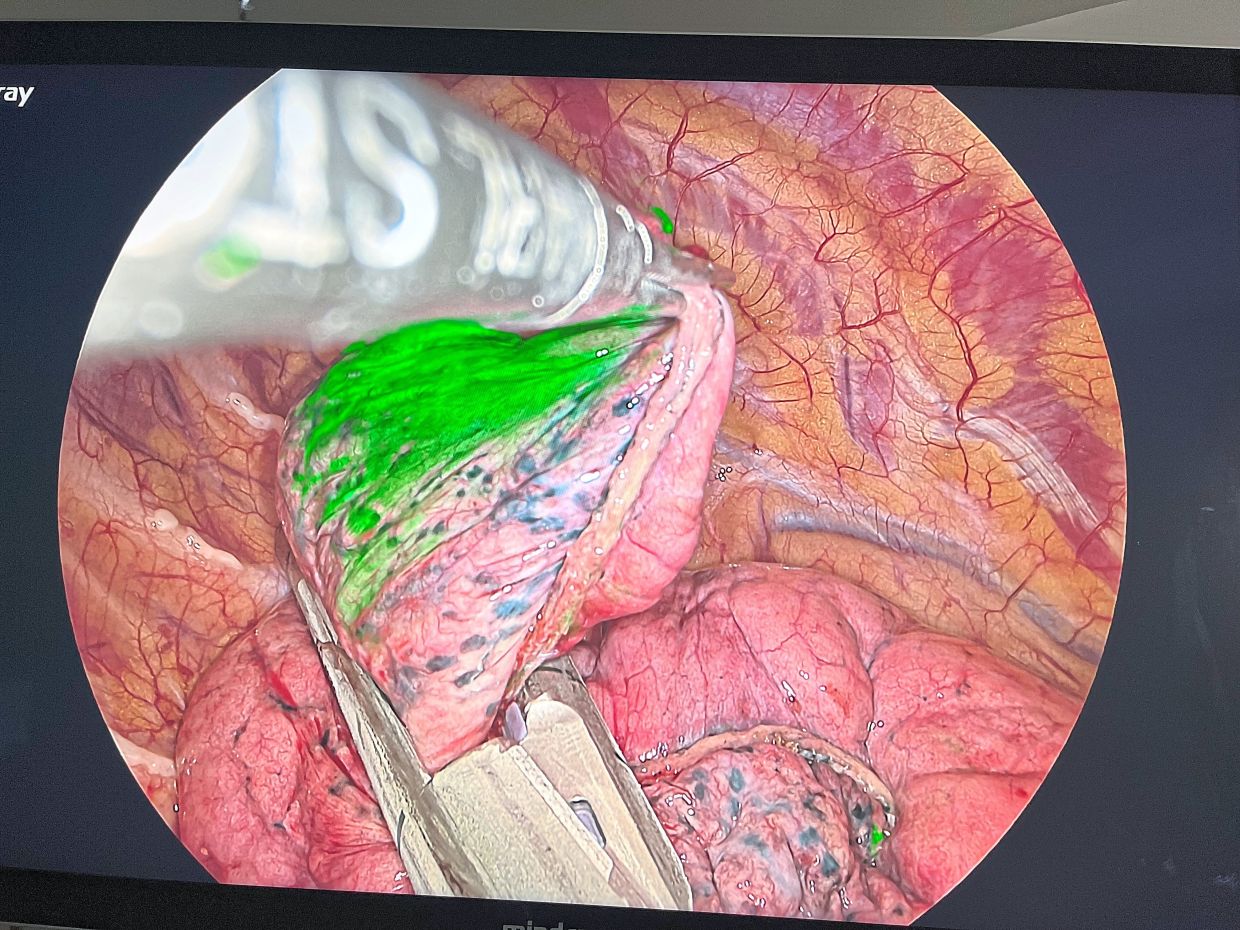
Too small to probe
Prof Anand explains: “Up until now, it’s hard to do anything for any nodule that is 1cm and smaller ... except wait for four to six months until the nodule grows bigger before it can be identified either by feel or visually, to be biopsied or removed with surgery.
“This wait creates considerable anxiety for both the patient and the doctor, and could waste precious time in initiating treatment for a possible cancerous lung tumour – be it primary or secondary.
“If it is benign, it may resolve by itself, stay the same or grow slowly. If it is cancerous, the nodule is going to grow rapidly and change its shape.”
Nodules that are small are difficult to reach due to the lung’s soft and spongy nature, which is filled with air sacs and delicate tissue, making a biopsy challenging.
Additionally, their deep-seated location and proximity to blood vessels can make them difficult to access and sample accurately.
The spongy lung structure itself can also cause a needle to move around, making it difficult to obtain a precise and stable sample, leading to a false negative result.
“The conventional method is to make a larger incision to put our fingers in to palpate. But finding the nodule can still be challenging as there are often no visual clues to guide the surgeon because the overlying lung tissue (parenchyma) may look deceptively normal.
“This is akin to looking for a tiny pea amidst a large spongy lung,” he says.
With the minimally invasive or keyhole uniportal video-assisted thoracoscopic surgery (VATS), the drawback is that surgeons cannot get their fingers in through a small incision.
Greater precision
Recently, a new technology using a special fluorescent dye called indocyanine green (ICG) has entered local practice.
ICG is a water- soluble non-toxic dye which emits a green signal under special imaging with near- infrared light.
With CT-guided imaging, an interventional radiologist will inject the ICG dye into the lung – near to but not into the nodule or suspected tumour – several hours before the planned surgery.
It’s important to inject into the correct area, as the purpose is to demarcate accurately so the surgeon can just remove the nodule without affecting much of the surrounding tissues.
“At surgery, the video telescope is introduced into the chest through a small incision. Once the special near-infrared light mode is activated (switching from the conventional white light setting), the injected area will light up in green to guide the surgeon on where to target.
“This enables the surgeon to safely and swiftly locate small and/or deeper nodules with precision.
“We then take a small segment of the nodule and send it to the pathologist while the patient is still under general anaesthesia.
“Within 15 minutes, the pathologist will tell us if it is benign or cancerous, and to assess the margins (i.e. if it has been fully removed with a cuff of healthy tissue),” explains Prof Anand.
He adds: “This is known as an intra-operative frozen section and will guide the surgeon on the next steps in the lung operation, which may involve removing more of the affected lung and in some cases, removal of lymph nodes in the chest cavity to give the patient the best chance of a cancer-free survival.”
Our right lung has three lobes while the left one has two.
The gold standard for treating lung cancer is a lobectomy, or the removal of the lobe of the lung that contains the nodule.
Unlike the liver, lung tissues do not regenerate.
“We only need one healthy lung to live well. The body is amazing, patients can still go back to hiking and everything else even when we have removed a third or half of the lungs.
“They don’t feel that missing part,” says Prof Anand.
All in one surgery
To date, approximately 15 such cases have been performed in the country using this new method.
Prof Anand shares his experience from two recent successful cases; both were young patients with prior cancers.
One had a treated colorectal cancer and the other, a treated cancer of the cervix.
On a routine surveillance PET (Positron Emission Tomography) scan, a small lung nodule was found in each patient.
He says: “In both cases, the nodules were malignant metastatic tumours from their original colon and cervical cancers, respectively.
“Hence, both operations were diagnostic, prognostic (staging) and therapeutic, and all done at one sitting. In these cases, it was Stage 4.”
The technology, which is also being used in other medical specialities, facilitates a single, minimally invasive approach, which allows patients to recover better and start further cancer treatment, if necessary.
“It involves a multi-disciplinary approach and close collaboration between the surgeon, interventional radiologist, pathologist and anaesthetist, highlighting the importance of teamwork and good communication.
“Aside from nodule localisation, the use of ICG may also help to delineate important structures and tissue planes for more complex procedures,” he concludes.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


