



Inflammatory bowel disease (IBD) encompasses chronic inflammatory conditions of the gastrointestinal tract (GI), primarily Crohn’s disease and ulcerative colitis (UC).
These conditions result from an abnormal immune response, leading to prolonged inflammation and damage to the digestive tract.
Crohn’s disease can affect any part of the GI tract from mouth to anus and often involves all layers of the bowel wall.
UC, on the other hand, is confined to the colon and rectum, affecting only the innermost lining.
Symptoms include persistent (more than one month) diarrhoea with mucus per rectum; abdominal pain, usually accompanied with rectal bleeding especially in UC; weight loss; and fatigue.
Some individuals may also experience extraintestinal manifestations like eye redness, joint pain or skin rashes.
In Malaysia, IBD was once rare but has seen a significant increase.
A local study from Hospital Canselor Tuanku Muhriz UKM in Kuala Lumpur, reported a rise in incidence from 0.36 per 100,000 person-years in the 1980s to 1.46 per 100,000 person-years between 2010 and 2018.
Globally, the prevalence is higher, with the United States reporting a rate of 721 per 100,000 person-years.
There is still lack of awareness on IBD among the public and general physicians in Malaysia, which inevitably leads to late diagnosis of the disease.
To complicate this further, IBD has multiple common mimics especially infectious colitis such as Mycobacterium tuberculosis.
Let’s shed some light on the challenges faced by patients with IBD.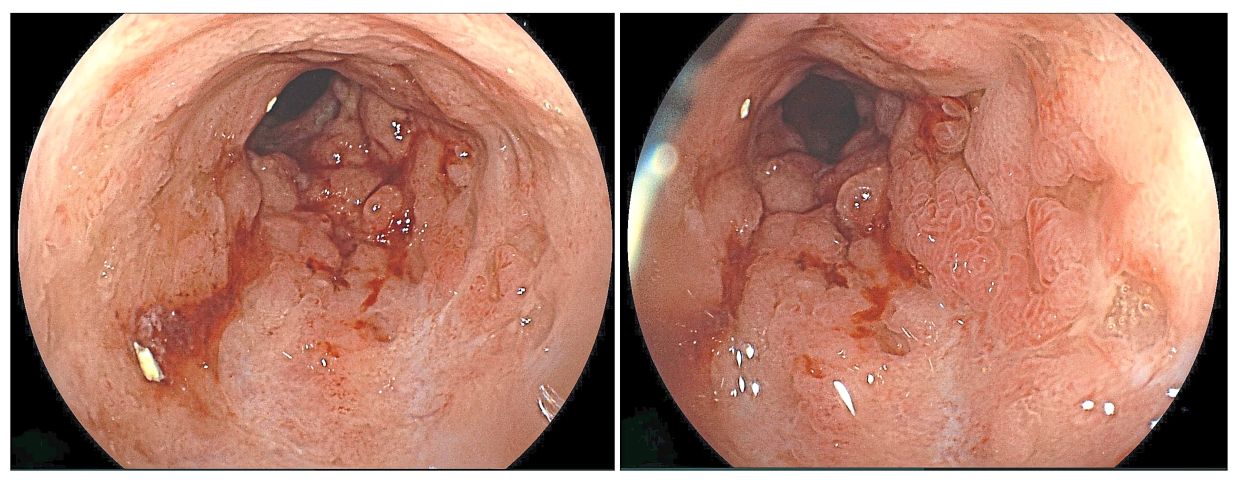
Silent struggle
One of my patients, Hairi, is a 42-year-old professional who was diagnosed with UC many years ago.
His battle with UC began subtly, with symptoms that were easy to dismiss.
Over the course of two to three months, Hairi noticed a persistent presence of white mucus in his stool.
Initially intermittent, the symptoms gradually became more frequent, culminating in rectal bleeding.
This alarming development marked a turning point, prompting him to seek medical attention.
The initial stages of diagnosis were fraught with uncertainty.
Hairi’s symptoms, resembling common gastrointestinal issues like diarrhoea and mild stomach discomfort, did not immediately signal a more serious condition.
However, the worsening bleeding led him to consult a general practitioner.
The initial assessment pointed to the possibility of colon cancer, a sobering thought that loomed over Hairi until he was referred to a gastroenterologist for further evaluation.
After doing a colonoscopy and subsequent biopsy, his diagnosis was confirmed: UC.
The road to managing his condition was anything but smooth.
At the height of his illness, Hairi faced debilitating symptoms that severely impacted his daily life.
Frequent bathroom trips – up to 15 times a day – made it nearly impossible to maintain a semblance of normalcy.
College life became unmanageable as he struggled to adhere to a strict diet of plain foods like white bread, boiled chicken, eggs and white rice.
Ultimately, he was forced to drop out of his studies, a decision that was both heartbreaking and unavoidable.
The lack of understanding from those around him compounded his struggles.
Family members dismissed his condition as a simple stomach issue, while some friends attributed his challenges to psychological factors.
This pervasive misunderstanding isolated Hairi further, robbing him of the support network he so desperately needed.
Social outings became rare, dietary restrictions tightened and the pursuit of relationships or career goals seemed like distant dreams.
His quality of life plummeted, leaving him feeling as though he had failed at life itself.
The emotional toll was immense, with feelings of shame and despair becoming constant companions.
Hairi’s invisible illness presented additional challenges.
Outwardly, he appeared healthy, leading many to underestimate the severity of his condition.
Those who eventually learned of his illness often distanced themselves, leaving only a few steadfast individuals to offer genuine support.
Fear of stigma also shaped his professional life; Hairi chose not to disclose his condition to his employer, aware of the potential for discrimination.
The weight of his illness even affected his self-perception, making him doubt his suitability for relationships or marriage.
Amidst these challenges, Hairi’s resilience shone through.
A friend once expressed admiration for his determination to fight for a degree, a career and a semblance of normalcy.
This encouragement stayed with Hairi, serving as a beacon of hope during his darkest moments.
Hope in clinical trial
This turning point came three years ago when Hairi was included in a blinded clinical study for a new biologic treatment.
The results were nothing short of life-changing.
From requiring up to 15 bathroom visits a day, Hairi’s condition improved dramatically, reducing his needs to just twice daily on most days.
This newfound stability allowed him to regain energy, expand his dietary options and rediscover the joys of life.
For the first time in years, he could travel, work and engage with the world beyond the confines of his illness.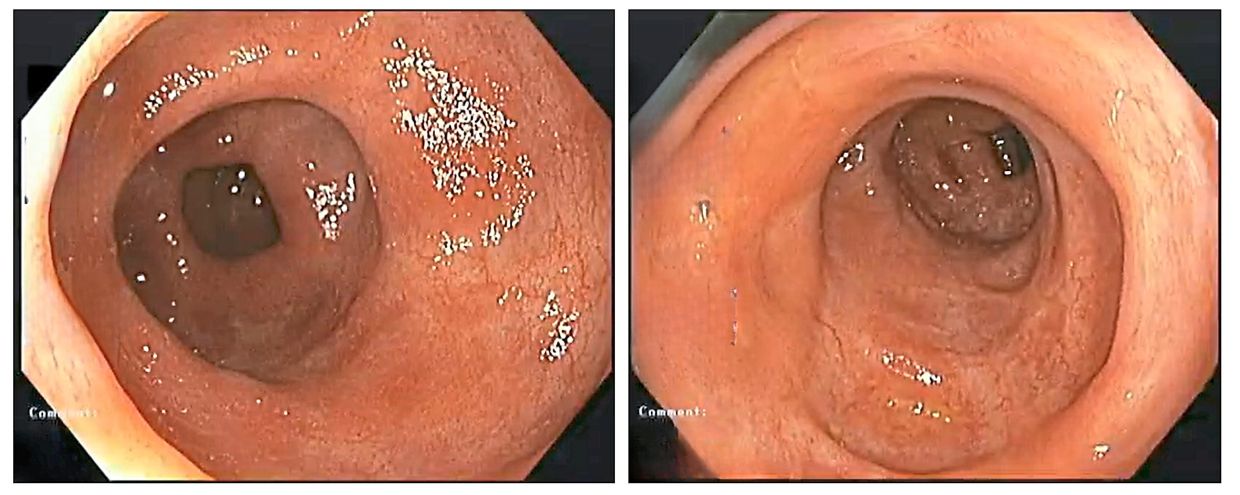
Hairi’s experience underscored the importance of regular follow-ups with a gastroenterologist and adherence to a treatment plan.
UC affects each patient differently, necessitating tailored approaches to management.
Regular check-ups provided a means to address diverse symptoms – from fatigue and low blood count to food sensitivities and skin rashes.
Treatment was not a quick fix but a long-term commitment requiring patience, consistency and effort.
Yet, with the right care and support, improvement was possible.
Despite the immense physical, emotional and social challenges posed by patients with IBD, Hairi emerged stronger, determined to live a fulfilling life.
Hope and healing are indeed possible.
An important issue highlighted by Hairi was the stigma surrounding IBD.
Despite being a medical condition with biological and immunological roots, IBD still carries a social stigma – especially in Malaysia and other Asian cultures where bowel-related issues are considered taboo or embarrassing.
So, what can we do?
Talk about it
Open conversations and educational initiatives are vital.
By discussing IBD more widely, the stigma surrounding it can be dismantled, creating an environment where patients feel understood and accepted.
Encouraging empathy is another crucial step.
Understanding its impact on daily life can inspire compassion and support from family, friends and colleagues.
Inclusivity in workplaces, and public spaces is essential to accommodate the unique needs of individuals with IBD.
Employers and institutions must recognise the value of creating supportive spaces that prioritise the well-being of their employees.
Just because you can’t see it, doesn’t mean it’s not real.
Dr Khairul Najmi Muhammad Nawawi is a consultant physician, gastroenterologist and hepatologist. For more information, email starhealth@thestar.com.my. The information provided is for educational purposes only and should not be considered as medical advice. The Star does not give any warranty on accuracy, completeness, functionality, usefulness or other assurances as to the content appearing in this column. The Star disclaims all responsibility for any losses, damage to property or personal injury suffered directly or indirectly from reliance on such information.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


