



How do you resolve the problem of having too much pressure within the head, i.e. intercranial pressure?
Doctors will first try giving medications to reduce the swelling or drain the extra cerebrospinal fluid or bleeding around the brain, depending on the cause of the condition.
If those methods fail, then removing part of the skull (craniotomy) is necessary.
Explains consultant neurosurgeon Dr Sharon Casilda Theophilus: “When you have a head injury or anything that increases intercranial pressure and affects your overall consciousness, we remove part of the skull bone.
“The skull is a rigid structure, unlike the body, which can expand with increased pressure.
“With too much pressure, the patient can go into a coma.
“We don’t want the coma to become irreversible, so one of the ways to release the pressure is to remove the bone flap for the brain to expand.”
Increased intercranial pressure can result from bleeding in the brain, a tumour, stroke, aneurysm, high blood pressure, a traumatic brain injury or brain infection.
“If you have seen strangers with a sunken skull, it’s likely that the bone flap has been removed; this is common with traumatic brain injuries.
“Even if you have a myocardial infarction (heart attack) and the brain swelling (oedema) is bad, causing you to become unconscious, we remove the bone flap to save lives,” she adds.
When the brain swells, it can be life-threatening, as it can constrict blood supply and destroy additional brain tissue.
Sometimes, a patient is put in a medically-induced coma or deep state of unconsciousness so that the brain is able to rest and decrease the swelling, and hopefully, preventing brain damage from occurring.
This was the case for former F1 racing driver Michael Schumacher, who was placed in a medically-induced coma for 250 days after suffering a severe head injury in a skiing accident in 2013.
Although the German is believed to still be recovering, no one has seen him in public since the unfortunate accident, which saw him falling onto a rock.
Removal and preservation
In the past, surgeons used manual saws to remove the bone flap, but with advances in technology, they now use a special high-speed drill.
This piece of bone is then cryopreserved in a bone bank as it needs to be kept at a certain temperature to remain viable.
Most Malaysian public hospitals have bone-banking facilities to provide allograft bones for surgeries.
Dr Sharon says: “When there is no bone bank, e.g. in some third world countries, the bone is then temporarily implanted in the patient’s abdominal tissue.
“It’s put there so that it can still receive adequate blood supply.
“Once the brain oedema is settled and the patient is recovering, and we notice that the brain is sunken, we put the bone flap back (cranioplasty).”
As one of the skull’s functions is to protect the inner contents of the head (i.e. the brain), any “sinkhole” needs to be covered.
Unlike fractures in limbs, which can be easily fixed with a cast, screws and pins, the skull requires a different approach.
“The longer I delay reconstructing the bone, the more the patient is affected.
“Without skull coverage, if the patient goes out in hot or cold weather, there will be discomfort or pain.
“And if he falls, he could injure his brain directly,” she says.
Some patients may also develop trephination syndrome, where neurological deterioration occurs following removal of a large skull bone flap.
The neurological status of the patient can also occasionally be related to pressure.
Dr Sharon says: “Because there is pressure from outside to inside, the patient may develop cognitive impairment, which improves when we put back the bone flap as it normalises the cerebrospinal fluid.”
Long-term effects

The timeline to put back the bone flap varies depending on where it is stored.
Normally, surgeons try to do it within six months.
Some freezers can store the bone well for up to two years, and others, a shorter duration.
“If you implant in the abdomen, the reconstruction needs to be performed earlier as the bone flap can dissolve.
“If you’ve done surgery elsewhere, sometimes the bone is not given back, or in the case of multiple fractures, it’s difficult to piece them back because they’re like a jigsaw puzzle.
“Also, the viability of the bone becomes questionable as we don’t know if it will actually fuse back,” says Dr Sharon.
In paediatric (child) groups, due to their fast growth rate, it’s common for the autologous (own) bone to get reabsorbed.
She explains: “After putting the bone in, within two months, there might be a defect again.
“You need good scaffolding between the autologous and present bone for the blood to reach back to the autologous bone for it to calcify.”
This scaffold commonly came in the shape of acrylic or titanium mesh, which were used to hold the bone together.
However, both materials have their own drawbacks.
“With acrylic, the issue is tissue incompatibility, i.e. the patient develops a reaction to the acrylic, causing him to have an infection or fluid collection at the surgical site, so it’s actually failure,” she points out.
Since the early 2000s, government hospitals have been using titanium mesh instead of acrylic.
This worked well, but over time, Dr Sharon, a former consultant at Sultan Aminah Hospital in Johor Baru, Johor, saw Singaporean patients coming to her clinic with the mesh protruding outwards from the skull.
She explains: “Singapore started using titanium earlier – in the 1990s.
“Some patients who lived there have now retired and moved to Malaysia; they were coming to hospitals with this problem.
“Imagine, you have a metal called titanium in your head, and years later, as your skin thins, it becomes exposed.
“So we have to take out this mesh and find another option – ideally, a material that is closest to mimicking our own bone.
“Then the failure rate is lower, there is less reaction to the skin, and it conforms to a better, natural shape.”
This is where tissue-generating technology comes in.
New technology
According to Osteopore Singapore’s chief technology officer Dr Jing Lim, the basis of tissue engineering lies in three parts: scaffolds, cells and growth factors.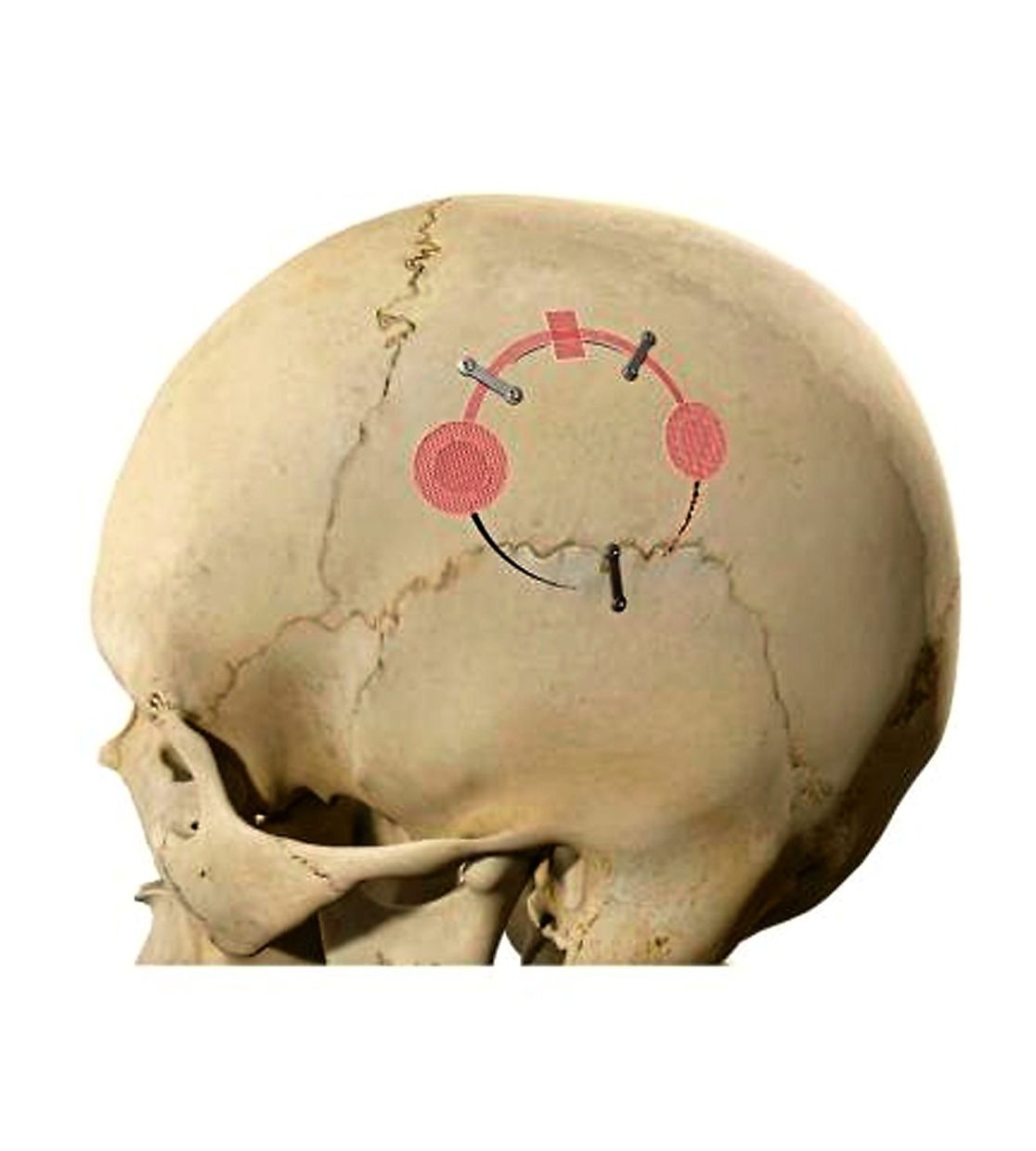
Tissues can easily be engineered in a lab: culture them in a petri dish, put them in a bioreactor, and over time, they grow into a piece of tissue.
“Whether it’s functional is a different question.
“There is a significant gap that a lot of technologists don’t get to cross, i.e. when they try to clinically translate this concept and apply it in a clinical setting.
“We developed the technology around scaffold components because the body has cells and growth factors, so it can take care of those.
“We chose polycaprolactone or PCL material, specifically because it degrades in the body and does it in a harmless way,” says the scientist.
A microstructure that resembles bone, which is non-porous on the outside, but porous on the inside, is then created via three-dimensional (3D) printing technology.
Dr Lim, who is also Osteopore’s chief operating officer, says: “We combine it with the scaffold, and thereafter, doctors and their teams come in with surgical techniques of either adding blood or bone marrow aspirate to the device.
“That completes the entire tissue engineering concept, which we can then apply clinically.”
The scaffolds, which are customised according to the shape and curvature required, stimulate bone growth so that the missing parts can be forged together.
Once the tissue and bones are successfully regrown, the scaffold dissolves into water and carbon dioxide in roughly 18-24 months, and is absorbed into the body.
Unlike conventional implants, there is no foreign material left in the patient’s body.
Tissue engineering can either be done in-vitro (inserting fabricated tissue into the affected area) or stimulated in-situ (harnessing the body’s regenerative abilities to rebuild lost or damaged tissues).
A more natural solution
In a world first and breakthrough in tissue engineering, surgeons managed to regrow a whole skull of an Australian man, who suffered traumatic brain injury and a severely broken leg from a motorcycle accident in 2019.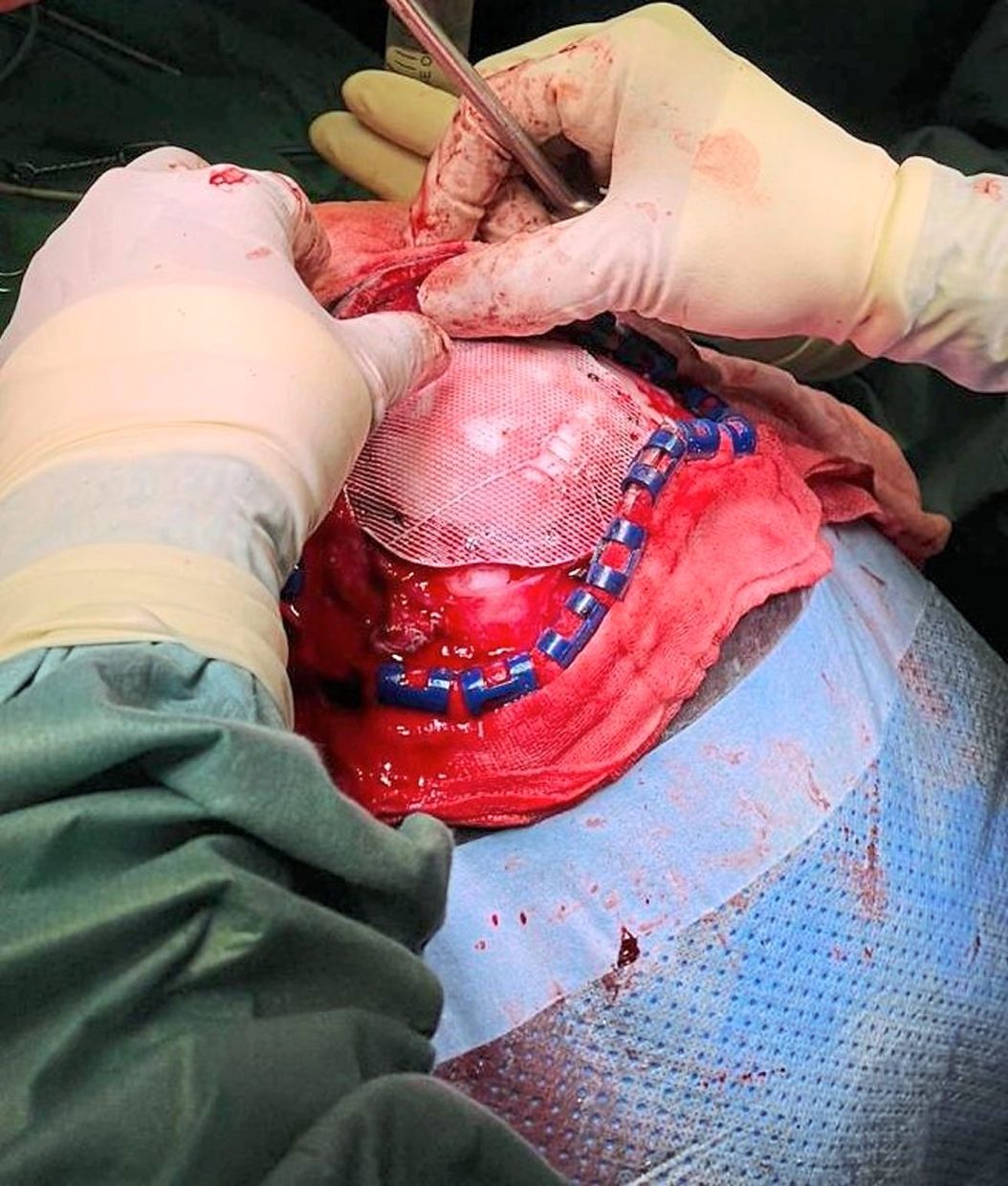
The scaffold was provided by Osteopore.
Dr Sharon gives the scenario of having to recreate half a skull: “If half the skull is taken out, we do a special computerised tomography (CT) scan and send it to Osteopore.
“Before, as we wouldn’t have brain images prior to the accident, we would do a 3D conformation based on the opposite side of the skull and recreate the missing half.”
Once she sends the CT scan to Dr Lim, his team figures out how to create the scaffold, using software.
The process of creating, sterilising and delivering the scaffold to the doctor takes about 10 days.
So far, as the first female neurosurgeon to practise in Malaysia, Dr Sharon has observed good results from tissue engineering, which she has been using for almost a decade.
She hasn’t come across any side effects or cases of rejection.
“The only problem we might face is that the scaffold gets absorbed too fast, before it can completely cover the defect.
“But since there is already a covering, which also calcifies over time, we don’t do anything and let it heal naturally,” she says.
This method is a better option for paediatric patients as it allows the child’s bone to grow.
She says: “If we use titanium mesh, it will impede the bone growth and the child may end up with a defect again.
“For adults, we give options depending on the size of defect.
“In the elderly with recurrent infections or if the skin is already thinned out, we suggest this option.
“We don’t want to disturb the normal physiology of the environment too much, and no, hair growth is not affected.”
Most of the time, the defects are high up in the head and need to be covered.
“Scaffolds are used for cosmetic reasons (you don’t want a sunken skull), to alleviate memory loss, and for safety.
“As a surgeon, my apprehension is whether the bone will grow back.
“To date, my experience with 3D scaffolds has been good, but as the technology is only about 10 years old, we have to wait to see,” she says.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


