



There are over a trillion nerves in the human body.
They serve as electrical wiring that transmits signals between the brain, spinal cord and the rest of the body.
At times, they can “short-circuit” and become pinched, squeezed or compressed, causing numbness, tingling, weakness and pain.
A pinched nerve can happen at any body part; a nerve that often gets compressed at the wrist is the median nerve.
When this happens, it’s called carpal tunnel syndrome (CTS).
CTS is a common form of nerve entrapment people often get due to repetitive motions such as typing.
The median nerve involved, and the surrounding nine tendons that bend the fingers, pass through the carpal tunnel – a narrow, rigid passageway at the base of the hand.
Sometimes, the thickening of the lining of the tendons (due to irritation or inflammation), or other types of swelling, narrows the tunnel and compresses the nerve.
As the median nerve provides sensation to the palm side of the thumb, index finger, second finger and part of the ring finger, these areas get affected.
The discomfort is usually worse at night, and the pain may stretch all the way from the wrist to the elbow.
The diagnosis is clinical: the surgeon takes the patient’s history and looks for risk factors, e.g. age/occupation, symptoms and pain site.
Patients are examined by tapping their wrists – a tingling sensation or electrical shock to the fingers are signs of CTS.
“The other way is to make them bend the wrist, and if they have similar symptoms as above or numbness in three fingers, then it is most likely the nerve impingement is at the wrist,” explains consultant hand and microsurgeon Dr Teh Kok Kheng.
“MRIs (magnetic resonance imaging) are not accurate.
“We can also do a nerve conduction test, i.e. put electrodes and run electricity in the nerve to measure how fast it is transmitted.
“It’s conducted in a lab and the results are interpreted by a neurologist.
“Unfortunately, the test is not widely available in our country.”
He notes that more patients have been showing up at his clinic in the past six months, complaining of hand numbness over the last two years.
This is likely due to the movement control order when many had to work remotely using laptops and then developed CTS.
Releasing the nerve
The first line of treatment for any pinched nerve is conservative: rest, apply heat or ice packs, and pop painkillers.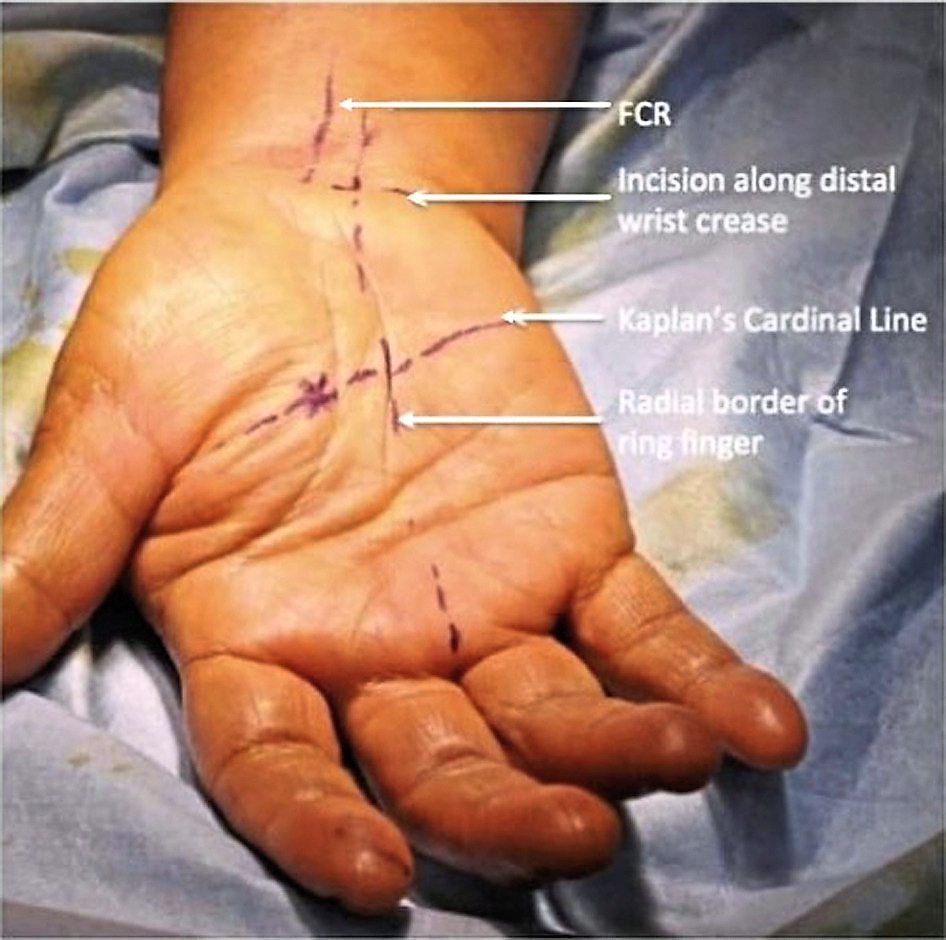
Depending on where the problem lies, you may also need to immobilise the area via a splint, collar or brace.
When all that fails, surgical intervention may be necessary.
An untreated CTS can lead to permanent dysfunction of the hand.
“Surgery is recommended in severe cases or where conservative treatment fails, i.e. the pain does not go off, the patient has recurring symptoms even after months of treatment, or there is a permanent change in the function of the hand.
“Because there is muscle wasting, there is a weakness in the thumb – the patient might say the hand feels weak when they write or they may drop something, even a light object,” says Dr Teh.
There are many surgical techniques out there to treat CTS and the traditional one is via an open carpal tunnel release.
This is where an incision is made at the wrist to cut the transverse carpal ligament and release the nerve from impingement.
Dr Teh explains: “It’s very simple: imagine wearing a shirt and your weight increases by 20kg – the shirt becomes tight.
“First, you try to exercise to shed the excesses to still fit into the shirt, but if you continue to gain weight, then you might struggle to breathe because the shirt has become too tight.
“So, you either unzip or unbutton the shirt, or cut at the sides, to be able to breathe.
“That’s what surgical intervention does; we cut the transverse carpal ligament (also called the flexor retinaculum) to create a bigger space in the tunnel so the nerve can ‘breathe’, but we don’t remove anything.”
With this open technique, the surgeon makes a blind cut on the transverse carpal ligament as they can’t see exactly where the nerve lies.
Hence, they make their best educated guess, which may sometimes end up injuring the surrounding structures.
The incision is long: around seven centimetres (cm) from the palm of the hand to 2-3cm up the forearm.
“The hand is very sensitive, therefore any wound on the palm takes time to heal, making the return to work time much longer,” he says.
He shares that his master’s thesis was on open CTR, which he performed on cadavers, explaining: “I was reluctant to perform it on patients as I had reservations about its safety.”
Guided by a camera
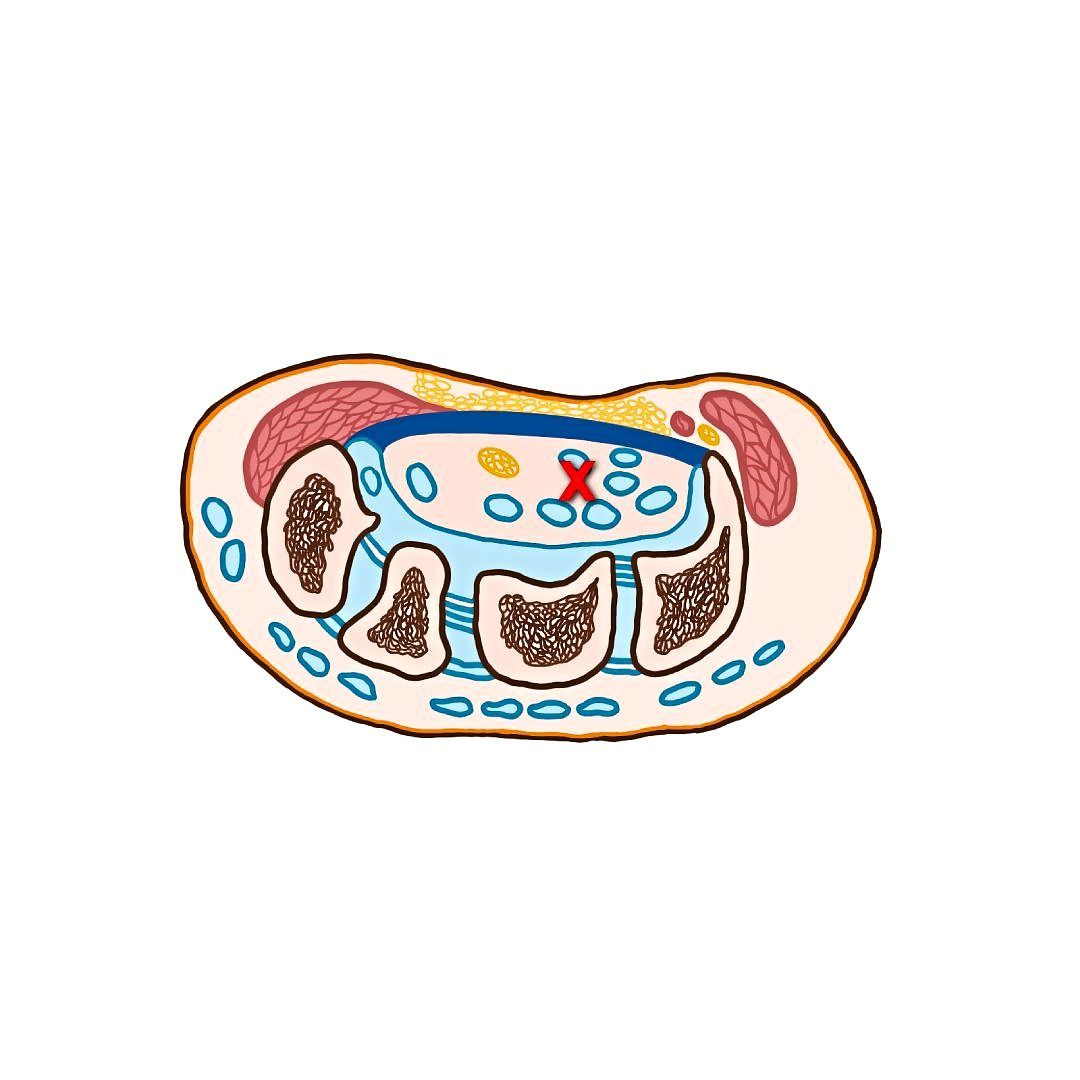
The other surgical method is endoscopic carpal tunnel release, in which a thin, flexible tube that contains a camera is inserted into the wrist through a tiny incision.
The camera guides the doctor as the surgery is done with thin tools put into the wrist through another small cut.
Dr Teh says: “Again, the problem is by putting a camera and other gadgets directly into a narrow tunnel (measuring around 8-10 millimetres, mm, at the wrist), the procedure can increase the risk of injuring the nerve.
“Therefore, not many surgeons use this technique.
“Master surgeons can do this well because they have gone through (practising on) tons of cadavers before performing the technique, but not every surgeon has that opportunity.
“Many people don’t want to learn new skills as they may have to ‘sacrifice’ a few patients before they can become masters, so they prefer doing the open CTR.”
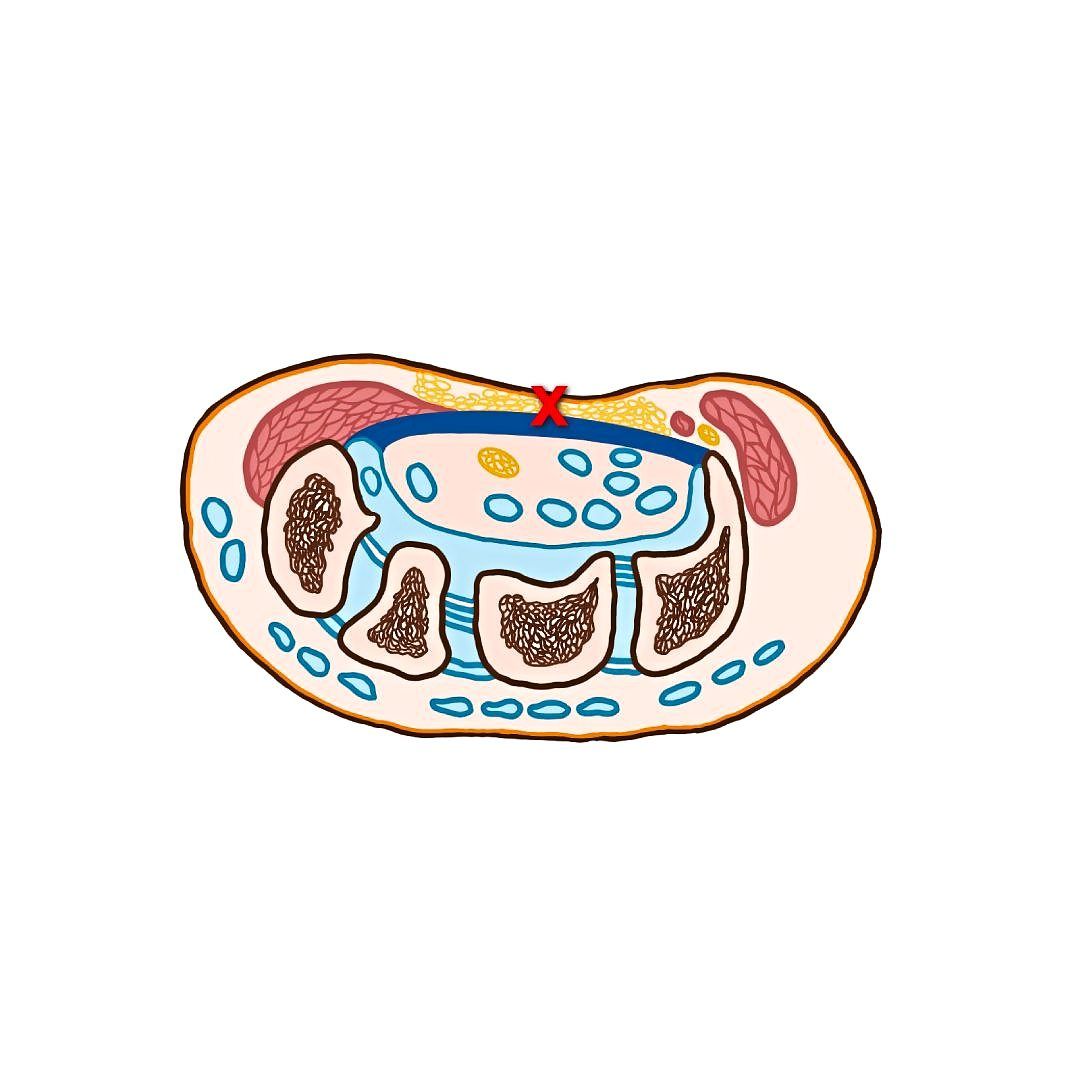
Years after this method was introduced, Australian hand and wrist surgeon Dr Jeff Ecker worked on refining it and came up with the Supra-Retinacular Endoscopic Carpal Tunnel Release (SRECTR).
In this technique, the endoscope and instruments are inserted above the transverse carpal ligament, which allows the surgeon to see the carpal tunnel without putting the median nerve at risk of damage during the surgery.
However, the instrument used was actually designed for endoscopic cubital tunnel release, i.e. for the release of a pinched nerve at the elbow.
“You are inserting an instrument of a 6-8mm diameter into the wrist, and this can increase intra-tunnel pressure and cause direct injury to the already injured median nerve,” Dr Teh points out, adding that he found the instrument too cumbersome.
Novel method
Dr Teh then poured his efforts into refining the SRECTR and came up with the supraretinacular retractor with L-bar.
After experimenting on over 300 cases, his final novel version of the SRECTR has the surgeon inserting the camera and instruments into the hand from above the transverse carpal ligament and below the skin.
“I am just pushing the skin away so I can see the transverse carpal ligament – underneath is the median nerve. In the old SRECTR technique, we can’t see the transverse carpal ligament as the camera is underneath it.
“I make an incision on the skin and create space using a pair of scissors, then the L-bar is inserted together with a 2.4 or 2.7mm endoscope into this space.
“You can see more structures and I am able to protect them,” he explains.
Dr Teh has patented this new technique, as well as authored a study on it, together with other local researchers, which was published in the Journal of Hand Surgery Global Online in 2021.
A total of 50 cases involving 46 patients (48 cases came back for follow-up, but the data for two cases were lost) were evaluated in the study.
All the surgeries were performed between 2016 and 2018.
The patients were evaluated before the surgery; at three, seven and 14 days after surgery; and at one, three and six months post-surgery.
The effectiveness of the surgery was evaluated, among others, using pinch and grip strengths, a modified table test, the visual analogue scale pain score, and the Disabilities of the Arm, Shoulder and Hand questionnaire.
All parameters showed improvement and there were no serious injuries or complications.
Dr Teh was thrilled.
“Before the results were published, I told my patients I was using my own technique to perform the CTR and I didn’t have any proof that it was better.
“We need to do randomised controlled trials for that.
“However, I believe it is better because they end up with a smaller scar (3-4cm) and can go back to function earlier,” he says.
The smaller wound allows the patient to use their hand earlier, i.e. seven to 10 days compared to 10-14 days with the open CTR.
It may not be a big difference, but it is a safer option.
The daycare surgery is done under local anaesthesia and takes around 40-50 minutes.
Open CTR takes 20-30 minutes.
In government hospitals, the open CTR is usually performed due to the lack of expensive instruments; the open CTR only requires a scalpel.
The surgical cost for an open CTS is roughly RM4,000, but with the novel SRECTR, the cost is double.
It can come back
Unfortunately, CTS can recur.
There are two types, says Dr Teh.
The first is real recurrence, where the patient gets better, but due to the development of scarring, the median nerve gets pinched again months or years later, causing the symptoms to recur.
This, however, is rare.
“The other type is that after surgery, there is no difference (for the patient),” he explains.
“This is because it has been wrongly diagnosed as CTS – perhaps it was a nerve impingement in the neck instead.
“Or during the surgery, the nerve was badly injured or the surgeon didn’t cut the transverse carpal ligament enough to fully release the nerve.”
He adds that this is why the endoscope is important: “We can see everything and fully release the nerve.”
From Dr Teh’s observation, once the nerve is released, it actually pops out and blood gushes back into it.
“I believe the nerve didn’t get enough nutrients, so it couldn’t sustain its function, hence it is painful,” he says.
On the topic of prevention, he believes that it is probably hard to prevent CTS as “all of us will age and our ligaments will stiffen”.
“But you can reduce your risk by taking frequent breaks from typing or using the handphone, and not use the wrist in a repetitive manner.
“Stretch out the fingers and hands, and that goes for everything: the back, neck, legs, etc,” he advises.
Already a subscriber? Log in
Get 20% OFF The Star Digital Access
Cancel anytime. Ad-free. Unlimited access with perks.


