



NEARLY 56,000 Malaysians suffer from end-stage kidney disease (ESKD), a condition under which a person’s kidneys have less than 15% of their normal function.
By 2040, experts estimate that the number of patients will nearly double to 106,000.
In the spirit of World Kidney Day 2026 which took place on March 12 this year, it is important to understand the current policy landscape for managing the national ESKD burden.
Currently, ESKD patients have three treatment options: kidney transplants, and two forms of renal replacement therapy (RRT), namely hemodialysis (HD) and peritoneal dialysis (PD).
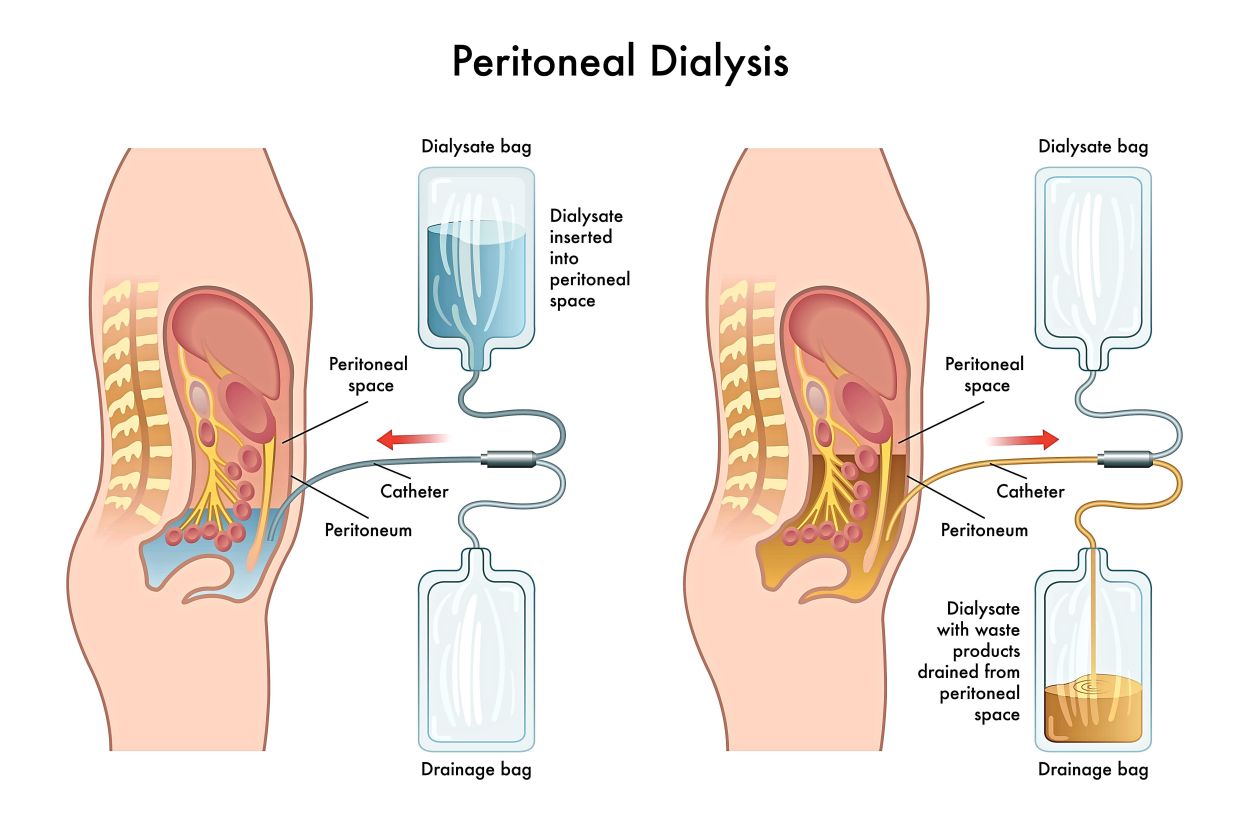
Hemodialysis is often conducted at centres; patients typically come into a HD centre three times a week and undergo treatment for several hours. PD is conducted in a home setting and utilises the patient’s own peritoneal lining in their abdomen as a natural filter to remove waste from the body.
EKSD patients undergoing either RRT will find themselves having to drastically adapt their work schedules, family responsibilities and travel plans to facilitate their treatment.
PD First as government policy
The Health Ministry (MOH) has a PD First policy, which, on paper, would put patients on PD first unless determined unsuitable by their doctor.
According to the Galen Center for Health and Social Policy, from a policy perspective PD requires less centre-based infrastructure and provides a scalable model to support RRT access in rural and underserved areas via home delivery.
Being a home-based modality also allows PD patients more flexibility in balancing their daily schedules around their treatment needs.
Published clinical literature shows that PD is associated with better preservation of residual kidney function, reduced cardiovascular stress, fewer risks of infection and offering similar survival rates to HD.
These, alongside the patient’s clinical context, become key factors in deciding on a suitable RRT.
Currently, both the MOH and other agencies such as the Social Security Organisation (PERKESO) fund programmes that provide Malaysians with access to continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis (APD).
As with all renal replacement therapies, patient suitability for PD is determined through clinical assessment by a treating specialist.
However, data from the 31st Report of the Malaysian Dialysis and Transplant Registry 2023 indicate a different reality than that proposed by the policy.
Although the MOH nominally has a PD First policy, home dialysis only accounts for 12% of patients, with the remaining 84% percent largely focused in HD.
On Jan 20, in a reply to Ampang MP Rodziah Ismail during a special chamber session, Health Minister Datuk Seri Dr Dzulkefly Ahmad reaffirmed the government’s commitment to a practical PD First policy.
The budget for PD will be more than doubled from RM40mil to RM100mil in fiscal year 2026.
The additional budget will be focused on increasing the number of PD patients in the public sector from 42% to 50% of the total ESKD patients under MOH.
While the expansion of the home dialysis policy programme is welcome, planning and execution should nonetheless account for ensuring the current supporting ecosystem remains robust with an influx of new patient initiations.
Overcoming patient anxieties with PD
Dzulkefly identified a lack of patient awareness of PD being a major obstacle to new patient initiation.
In his reply to Rodziah, he noted that patients might be anxious to start home-based treatment if they lacked proper infrastructure to maintain a sufficiently sterile home environment and store supplies.
Currently, patients covered under various government CAPD and APD programmes are already given training at PD-equipped centres close to their homes.
30-year-old housewife Nur Ainaa Syahirah Musa was prescribed CAPD in April 2025 after her kidney function had declined following childbirth and years of high blood pressure.
At Hospital Selayang, she was taught by the PD nurses on how to perform the treatment at home.
Over the following days, she grew more familiar with the process through the guidance of her care team.
Similarly, Giam Yee Fern, a 35-year-old professional learning and development trainer based in Kuala Lumpur, received similar training at Hospital Kuala Lumpur to undergo APD.
Both patients attend regular monthly checkups with their respective specialists, where any concerns with the treatment process are discussed with their care teams.
As the programme continues to scale, it will be key for the government to make sure patient experiences with the treatment remain consistent.
Home-delivery: a cornerstone of the PD First policy
The effectiveness of the PD First policy in providing equitable treatment access to patients is predicated on reliable and timely home delivery of supplies as well as improving connectivity between MOH facilities and the communities they service.
Working with reliable suppliers and logistics partners that are responsive to patient circumstances, particularly in remote and rural areas, becomes paramount.
Both Nur Ainaa and Giam affirm that they receive their monthly supply around the 20th day of each month, which are sent directly to their homes.
They coordinate these supply runs with the government-appointed logistics partners, who communicate by app and email.
This app allows patients to schedule deliveries and report issues like damaged stock.
To date, neither of them have ever experienced a late delivery.
As MOH scales its PD First policy, maintaining reliability in home delivery requires more careful planning and accounting for increased costs.
The ministry must mandate that suppliers maintain regular communication channels to coordinate deliveries and address any issues related to delivery scheduling and supply quality as part of programme oversight.

A supporting digital framework
In a similar vein, the MOH can also explore integrating technology that facilitates coordination between kidney care departments and the communities they serve. Many ESKD patients live in rural areas, far from where most health services are concentrated, and in parts of East Malaysia and the interior of Peninsular Malaysia, travel may even require boat transport.
For some patients, it can take up to an hour or more to reach the nearest MOH kidney care centre, and narrowing this distance - whether physical or digital - could meaningfully support policy goals.
For Nur Ainaa, for instance, it is a 90-minute drive from her residence in Kuala Kubu Baru to Hospital Selayang. A key opportunity for the ministry lies in strengthening digital infrastructure and capabilities.
This is especially timely as the PD First policy is being scaled up alongside ongoing efforts to digitise medical records and enhacne telehealth governance.
Building on the home-based nature of PD, policymakers can thoughtfully expand the use of secure, interoperable digital tools and common data standards that enable better coordination and continuity of care, particularly across wide rural catchment areas.
As the PD programme grows, MOH must place greater emphasis on resilient delivery systems, the integration of secure and interoperable digital infrastructure, and the use of clear operational benchmarks to ensure that day‑to‑day implementation keeps pace with national policy commitments.
Shazwan Mustafa Kamal
Regional Healthcare Lead
Vriens & Partners
Vriens & Partners is a government affairs consulting firm that actively supports advocacy efforts that improve healthcare policy.


